

Heterogeneities in the case fatality ratio in the West African Ebola outbreak 2013-2016
- PMID: 28396479
- PMCID: PMC5394646
- DOI: 10.1098/rstb.2016.0308
Heterogeneities in the case fatality ratio in the West African Ebola outbreak 2013-2016
Abstract
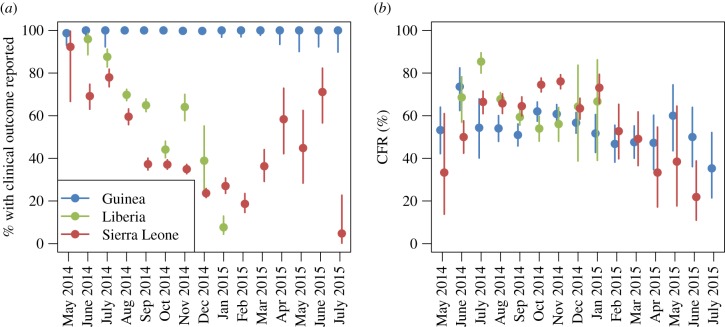
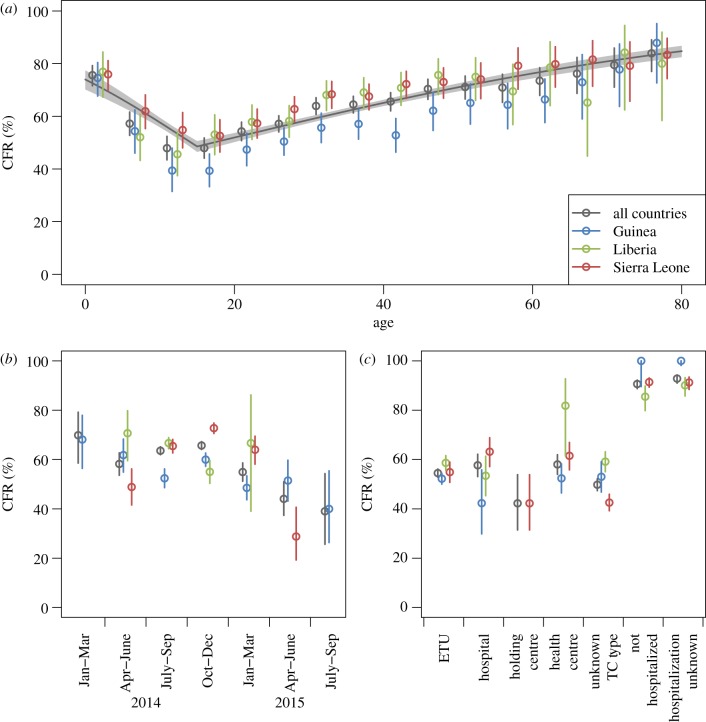
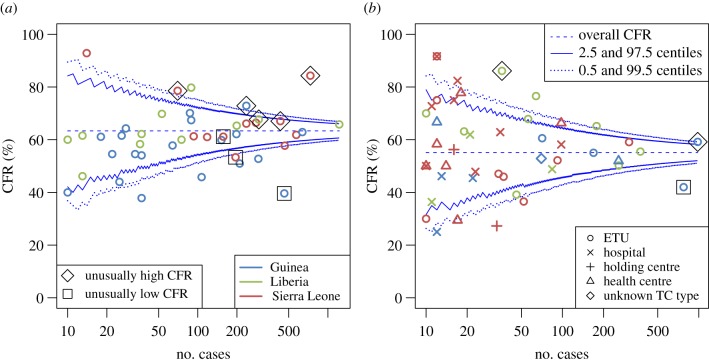
The 2013-2016 Ebola outbreak in West Africa is the largest on record with 28 616 confirmed, probable and suspected cases and 11 310 deaths officially recorded by 10 June 2016, the true burden probably considerably higher. The case fatality ratio (CFR: proportion of cases that are fatal) is a key indicator of disease severity useful for gauging the appropriate public health response and for evaluating treatment benefits, if estimated accurately. We analysed individual-level clinical outcome data from Guinea, Liberia and Sierra Leone officially reported to the World Health Organization. The overall mean CFR was 62.9% (95% CI: 61.9% to 64.0%) among confirmed cases with recorded clinical outcomes. Age was the most important modifier of survival probabilities, but country, stage of the epidemic and whether patients were hospitalized also played roles. We developed a statistical analysis to detect outliers in CFR between districts of residence and treatment centres (TCs), adjusting for known factors influencing survival and identified eight districts and three TCs with a CFR significantly different from the average. From the current dataset, we cannot determine whether the observed variation in CFR seen by district or treatment centre reflects real differences in survival, related to the quality of care or other factors or was caused by differences in reporting practices or case ascertainment.This article is part of the themed issue 'The 2013-2016 West African Ebola epidemic: data, decision-making and disease control'.
Keywords: Ebola virus disease; case fatality ratio; mortality; outlier detection; severity; spatial heterogeneity.
© 2017 The Authors.
Conflict of interest statement
We have no competing interests.
Figures
References
-
- World Health Organization. 2016. Situation report: Ebola virus disease, 10 June 2016. Geneva, Switzerland: World Health Organization.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical