

Percutaneous Pericardial Resection: A Novel Potential Treatment for Heart Failure With Preserved Ejection Fraction
- PMID: 28396500
- PMCID: PMC5390814
- DOI: 10.1161/CIRCHEARTFAILURE.116.003612
Percutaneous Pericardial Resection: A Novel Potential Treatment for Heart Failure With Preserved Ejection Fraction
Abstract
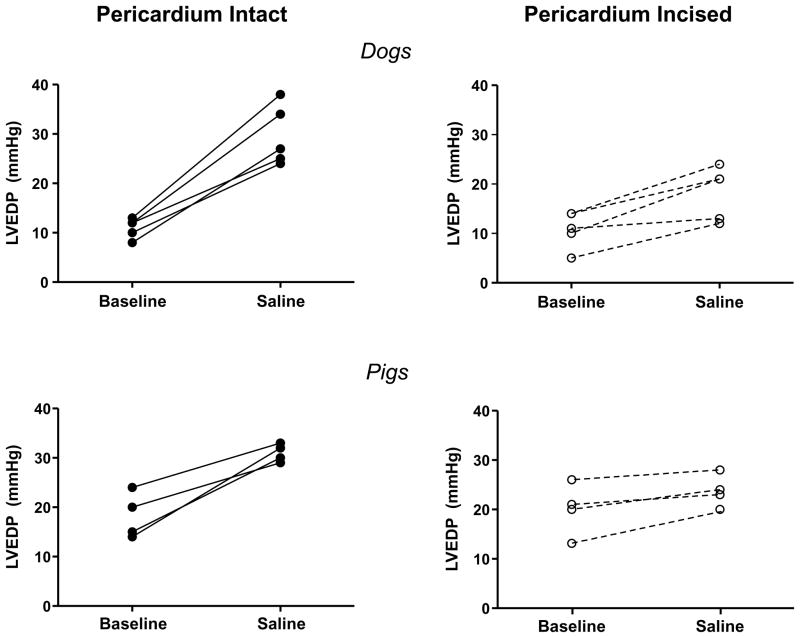
Background: People with heart failure and preserved ejection fraction develop increases in left ventricular (LV) end-diastolic pressures during exercise that contribute to dyspnea. In normal open-chest animal preparations, the pericardium restrains LV filling when central blood volume increases. We hypothesized that resection of the pericardium using a minimally invasive epicardial approach would mitigate the increase in LV end-diastolic pressure that develops during volume loading in normal and diseased hearts with the chest intact.
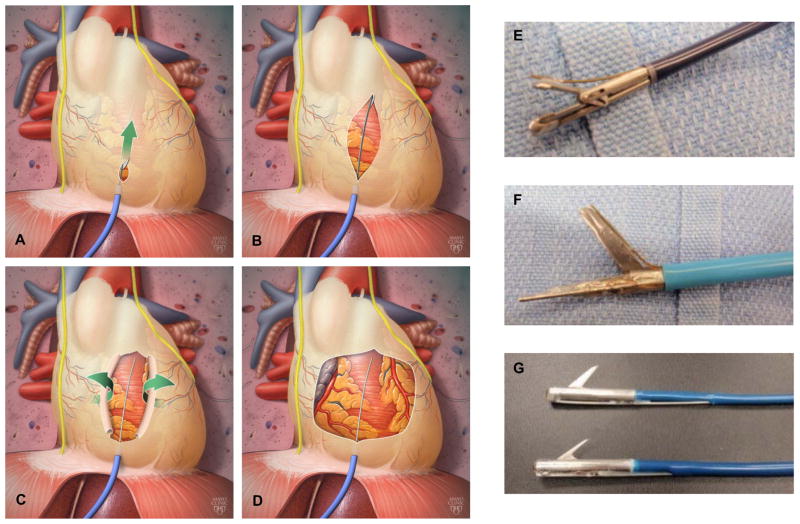
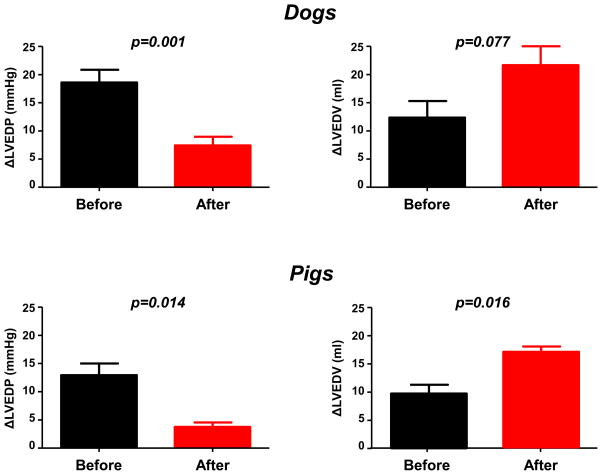
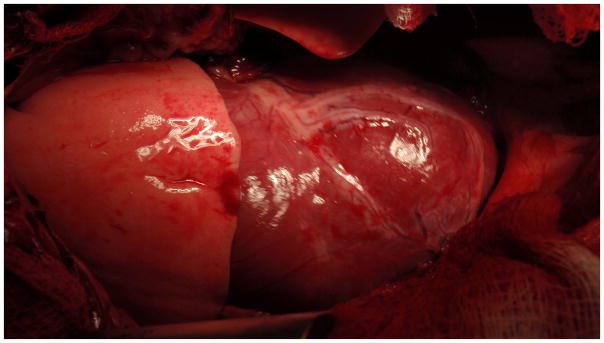
Methods and results: Invasive hemodynamic assessment was performed at baseline and after saline load before and after pericardial resection in normal canines with open (n=3) and closed chest (n=5) and in a pig model with features of human heart failure and preserved ejection fraction with sternum intact (n=4). In closed-chest animals, pericardiotomy was performed using a novel subxiphoid procedure. In both experimental preparations of normal dogs, pericardiotomy blunted the increase in LV end-diastolic pressure with saline infusion, while enhancing the saline-mediated increase in LV end-diastolic volume. With chest intact in the pig model, percutaneous pericardial resection again blunted the increase in LV end-diastolic pressure secondary to volume expansion (+4±3 versus +13±5 mm Hg; P=0.014), while enhancing the saline-mediated increase in LV end-diastolic volume (+17±1 versus +10±2 mL; P=0.016).
Conclusions: This proof of concept study demonstrates that pericardial resection through a minimally invasive percutaneous approach mitigates the elevation in LV filling pressures with volume loading in both normal animals and a pig model with diastolic dysfunction. Further study is warranted to determine whether this method is safe and produces similar acute and chronic hemodynamic benefits in people with heart failure and preserved ejection fraction.
Keywords: blood volume; heart failure; hemodynamics; humans; pericardium.
© 2017 American Heart Association, Inc.
Figures
Comment in
-
Pericardiectomy to Treat Heart Failure With Preserved Ejection Fraction: Unrestrained Enthusiasm?Circ Heart Fail. 2017 Apr;10(4):e003971. doi: 10.1161/CIRCHEARTFAILURE.117.003971. Circ Heart Fail. 2017. PMID: 28396502 Free PMC article. No abstract available.
References
-
- Paulus WJ, Tschope C. A novel paradigm for heart failure with preserved ejection fraction: Comorbidities drive myocardial dysfunction and remodeling through coronary microvascular endothelial inflammation. J Am Coll Cardiol. 2013;62:263–271. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
