

New-Onset Refractory Status Epilepticus with Claustrum Damage: Definition of the Clinical and Neuroimaging Features
- PMID: 28396650
- PMCID: PMC5366956
- DOI: 10.3389/fneur.2017.00111
New-Onset Refractory Status Epilepticus with Claustrum Damage: Definition of the Clinical and Neuroimaging Features
Abstract
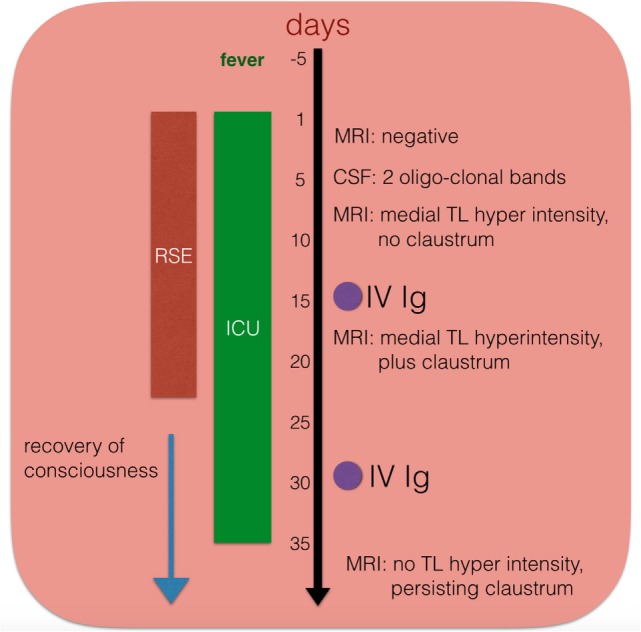
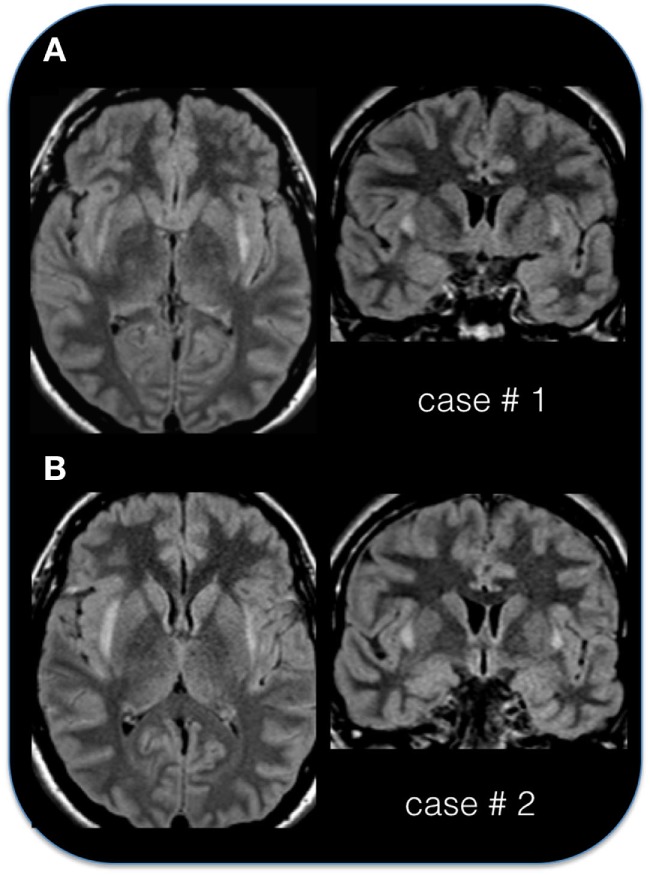
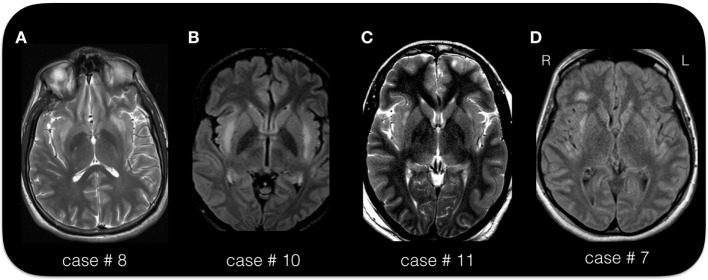
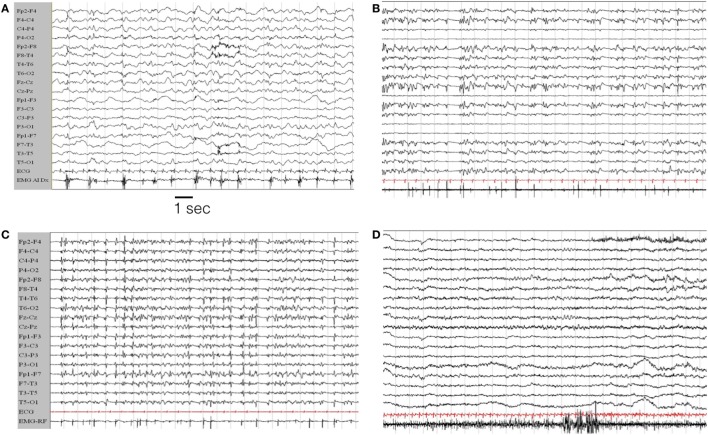
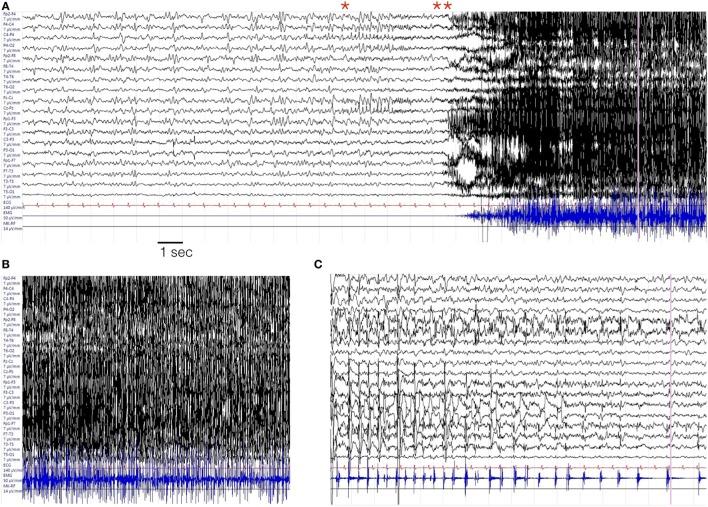
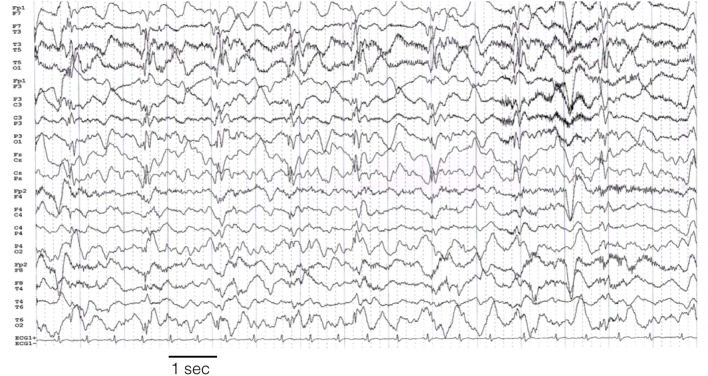
New-onset refractory status epilepticus (NORSE) is a rare but challenging condition occurring in a previously healthy patient, often with no identifiable cause. We describe the electro-clinical features and outcomes in a group of patients with NORSE who all demonstrated a typical magnetic resonance imaging (MRI) sign characterized by bilateral lesions of the claustrum. The group includes 31 patients (12 personal and 19 previously published cases; 17 females; mean age of 25 years). Fever preceded status epilepticus (SE) in 28 patients, by a mean of 6 days. SE was refractory/super-refractory in 74% of the patients, requiring third-line agents and a median of 15 days staying in an intensive care unit. Focal motor and tonic-clonic seizures were observed in 90%, complex partial seizures in 14%, and myoclonic seizures in 14% of the cases. All patients showed T2/FLAIR hyperintense foci in bilateral claustrum, appearing on average 10 days after SE onset. Other limbic (hippocampus, insular) alterations were present in 53% of patients. Within the personal cases, extensive search for known autoantibodies was inconclusive, though 7 of 11 patients had cerebrospinal fluid lymphocytic pleocytosis and 3 cases had oligoclonal bands. Two subjects died during the acute phase, one in the chronic phase (probable sudden unexplained death in epilepsy), and one developed a persistent vegetative state. Among survivors, 80% developed drug-resistant epilepsy. Febrile illness-related SE associated with bilateral claustrum hyperintensity on MRI represents a condition with defined clinical features and a presumed but unidentified autoimmune etiology. A better characterization of de novo SE is mandatory for the search of specific etiologies.
Keywords: claustrum; epilepsy; fever; new-onset refractory status epilepticus; refractory status epilepticus; status epilepticus.
Figures
References
-
- Van Lierde I, Van Paesschen W, Dupont P, Maes A, Sciot R. De novo cryptogenic refractory multifocal febrile status epilepticus in the young adult: a review of six cases. Acta Neurol Belg (2003) 103:88–94. - PubMed
-
- Wilder-Smith EP, Lim EC, Teoh HL, Sharma VK, Tan JJ, Chan BP, et al. The NORSE (new-onset refractory status epilepticus) syndrome: defining a disease entity. Ann Acad Med Singapore (2005) 34:417–20. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources