

A novel classification scheme for advanced laryngeal cancer midline involvement: implications for the contralateral neck
- PMID: 28396948
- PMCID: PMC11819287
- DOI: 10.1007/s00432-017-2419-1
A novel classification scheme for advanced laryngeal cancer midline involvement: implications for the contralateral neck
Abstract
Purpose: There are insufficient data concerning risk factors for contralateral regional metastases in laryngeal cancer. The aim of this study was to investigate the frequency and risk factors for contralateral lymph node metastases and their dependence on midline involvement of the primary tumor in patients with advanced laryngeal squamous cell carcinoma.
Methods: 58 consecutive patients (8 females, 50 males; mean age 64.2 ± 9.8 years; AJCC stage III disease in 43.1%, IVA disease in 54.4%) undergoing primary total laryngectomy with bilateral neck dissection between 2002 and 2016 have been retrospectively investigated at one of the largest university medical centers in Europe. Preoperative staging computed tomography (CT) scans were analyzed for midline involvement of the primary laryngeal cancer. As a result, a classification scheme has been established (type A: clear, type B: involved, type C: exceeded, and type D: bilateral/origin side indeterminable).
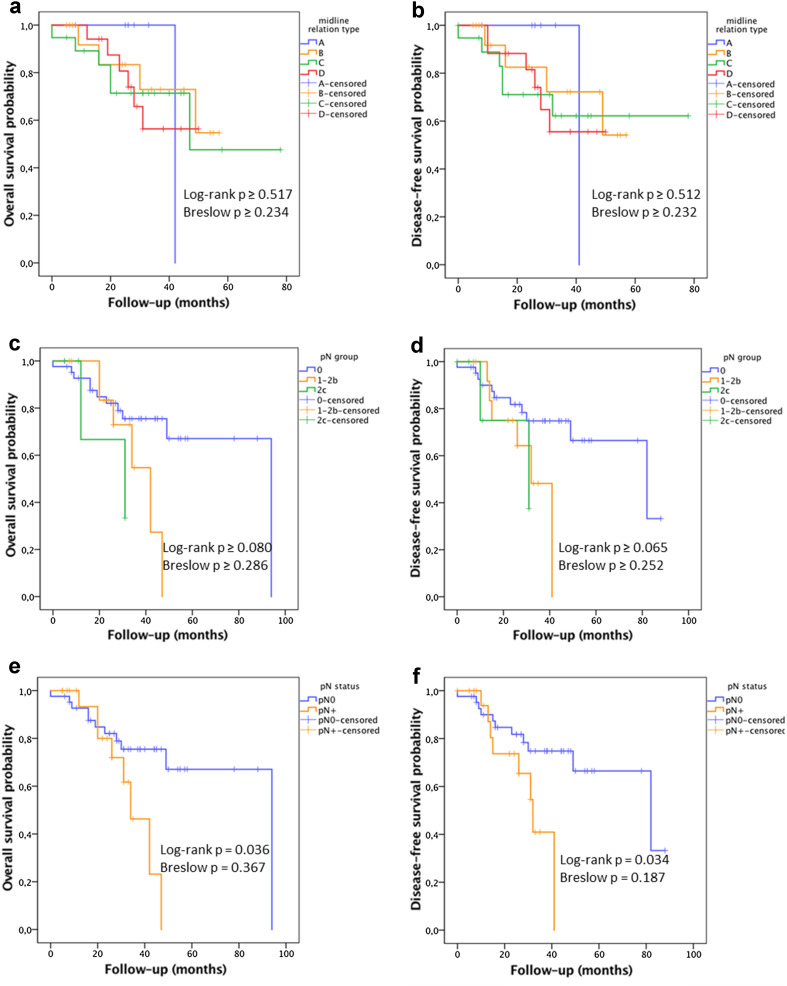
Results: Contralateral lymph node metastases (pN2c necks) were found in six cases (10.3%), from which four were diagnosed with type D (23.5% of type D cases), and one each with type B and type C midline involvement. In cases with no midline involvement (type A), a risk ratio reduction of 100% was seen. CT-based midline typing resulted in fourfold increased sensitivity for predicting contralateral metastases compared to conventional staging. Positive nodal status (pN+) significantly reduced overall and disease-free survival (HR 2.706, p < 0.05).
Conclusions: As a consequence, for type A category, a contralateral neck dissection might be avoidable accompanied by a reduction in surgical complications and operating time.
Keywords: HNSCC; Laryngeal cancer; Laryngectomy; Midline involvement; Neck dissection; Regional metastases.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

References
-
- de Bondt RB, Nelemans PJ, Bakers F et al (2009) Morphological MRI criteria improve the detection of lymph node metastases in head and neck squamous cell carcinoma: multivariate logistic regression analysis of MRI features of cervical lymph nodes. Eur Radiol 19(3):626–633. doi:10.1007/s00330-008-1187-3(Epub 2008 Oct 7) - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
