

Microbial shifts and signatures of long-term remission in ulcerative colitis after faecal microbiota transplantation
- PMID: 28398347
- PMCID: PMC5520032
- DOI: 10.1038/ismej.2017.44
Microbial shifts and signatures of long-term remission in ulcerative colitis after faecal microbiota transplantation
Abstract
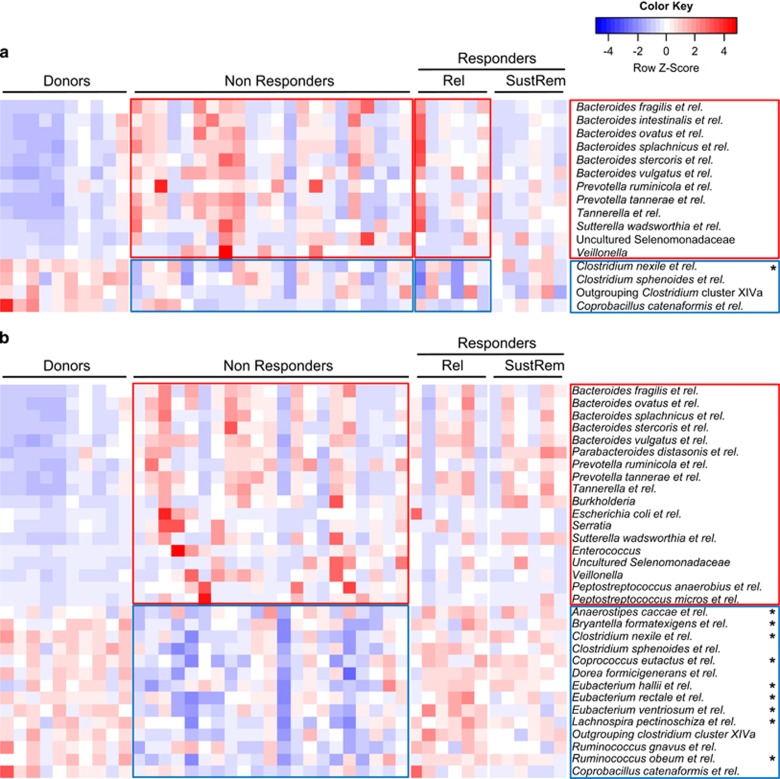
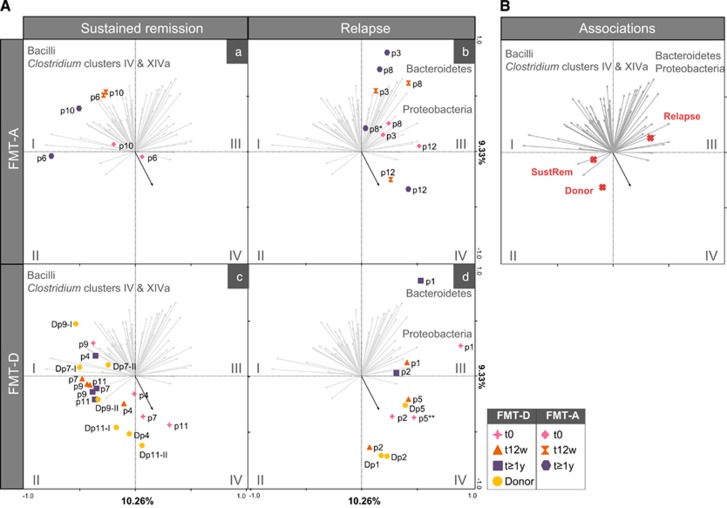
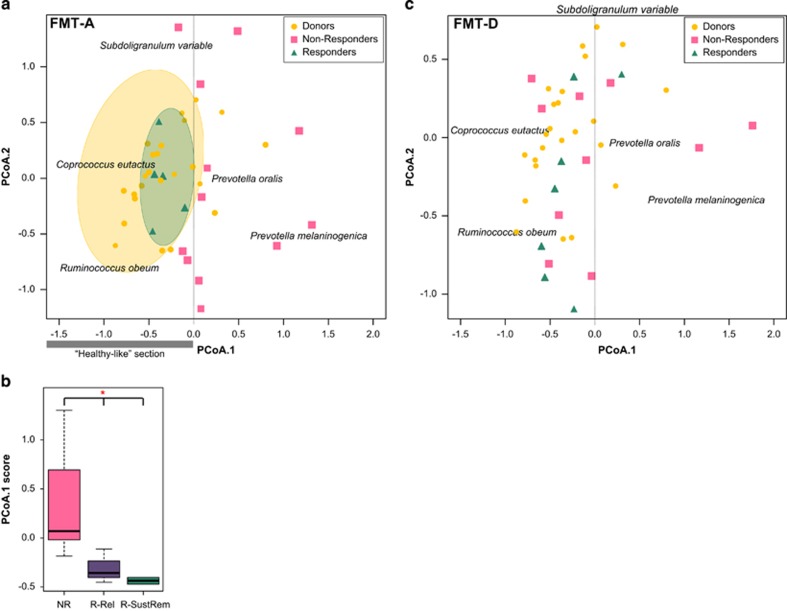
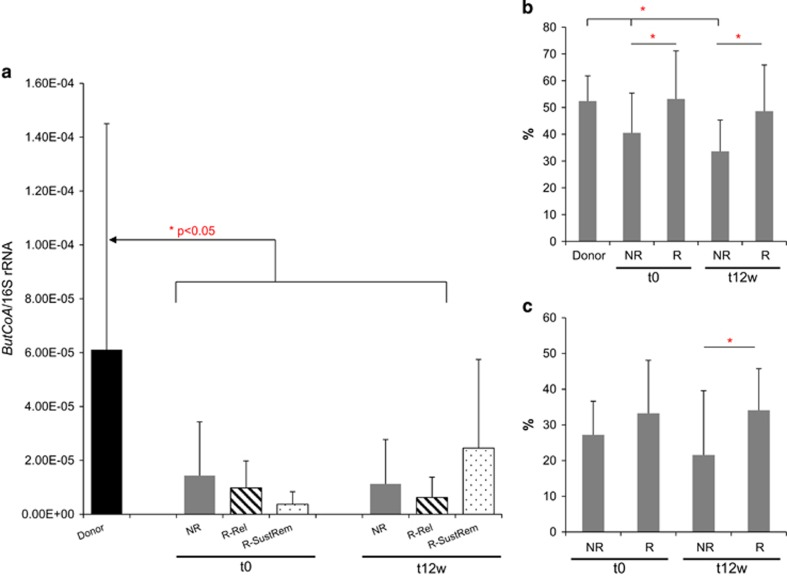
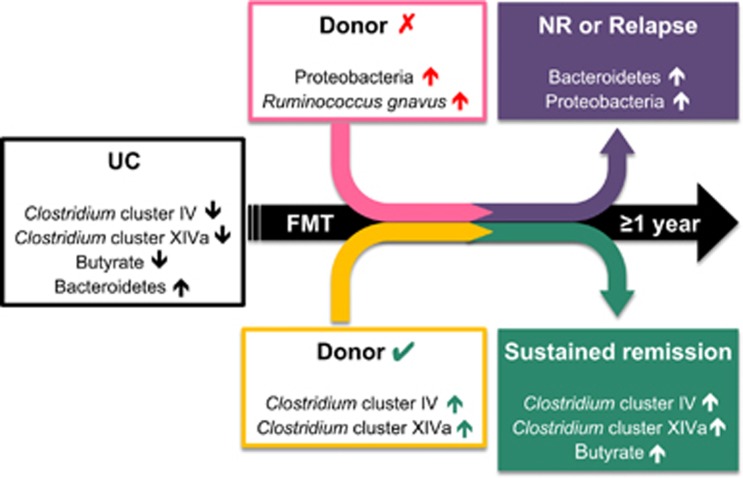
Faecal microbiota transplantation (FMT) may contribute towards disease remission in ulcerative colitis (UC), but it is unknown which factors determine long-term effect of treatment. Here, we aimed to identify bacterial signatures associated with sustained remission. To this end, samples from healthy donors and UC patients-grouped into responders and non-responders at a primary end point (week 12) and further stratified by sustained clinical remission and relapse assessed at ⩾1-year follow-up were analysed, comparing the efficacy of FMT from either a healthy donor or autologous faeces. Microbiota composition was determined with a 16S rRNA gene-based phylogenetic microarray on faecal and mucosal samples, and functional profiles were predicted using PICRUSt with quantitative PCR verification of the butyrate production capacity; short-chain fatty acids were measured in faecal samples. At baseline, UC patients showed reduced amounts of bacterial groups from the Clostridium cluster XIVa, and significantly higher levels of Bacteroidetes as compared with donors. These differences were reduced after FMT mostly in responders. Sustained remission was associated with known butyrate producers and overall increased butyrate production capacity, while relapse was associated with Proteobacteria and Bacteroidetes. Ruminococcus gnavus was found at high levels in donors of failed FMT. A microbial ecosystem rich in Bacteroidetes and Proteobacteria and low in Clostridium clusters IV and XIVa observed in UC patients after FMT was predictive of poor sustained response, unless modified with a donor microbiota rich in specific members from the Clostridium clusters IV and XIVa. Additionally, sustained response was associated with restoration of the butyrate production capacity.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Angelberger S, Lichtenberger C, Gratzer C, Papay P, Primas C, Eser A et al. (2012). P374 Fecal transplantation in patients with moderately to severely chronic active ulcerative colitis (UC). J Crohn's Colitis 6: S159–S159.
-
- Aroniadis OC, Brandt LJ, Greenberg A, Borody T, Kelly CR, Mellow M et al. (2016). Long-term follow-up study of fecal microbiota transplantation for severe and/or complicated Clostridium difficile infection: a multicenter experience. J Clin Gastroenterol 50: 398–402. - PubMed
-
- Basset C, Holton J, Bazeos A, Vaira D, Bloom S. (2004). Are Helicobacter species and enterotoxigenic Bacteroides fragilis involved in inflammatory bowel disease? Dig Dis Sci 49: 1425–1432. - PubMed
-
- Benjamini Y, Hochberg Y. (1995). Controlling the false discovery rate—a practical and powerful approach to multiple testing. J R Stat Soc Ser B 57: 289–300.
-
- Berry D, Reinisch W. (2013). Intestinal microbiota: a source of novel biomarkers in inflammatory bowel diseases? Best Pract Res Clin Gastroenterol 27: 47–58. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
