

Pharmacogenomics-Based Point-of-Care Clinical Decision Support Significantly Alters Drug Prescribing
- PMID: 28398598
- PMCID: PMC5636653
- DOI: 10.1002/cpt.709
Pharmacogenomics-Based Point-of-Care Clinical Decision Support Significantly Alters Drug Prescribing
Abstract
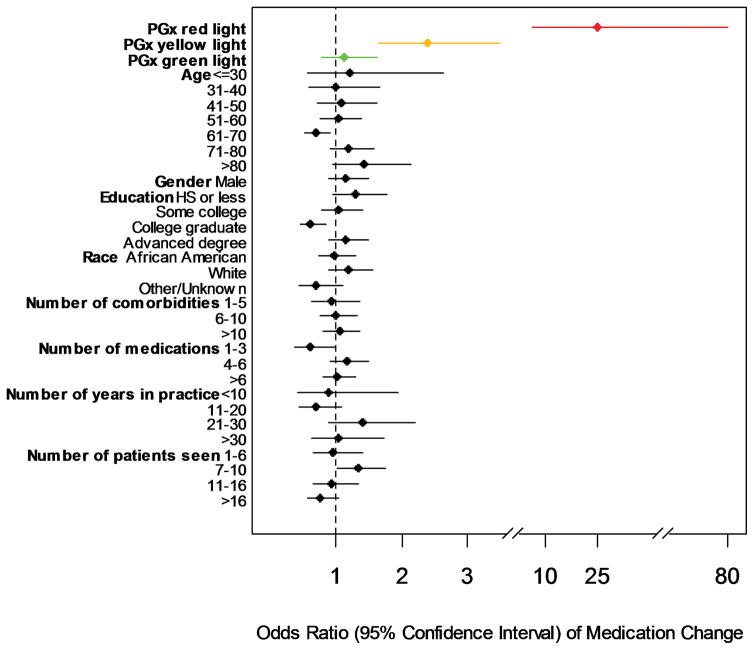
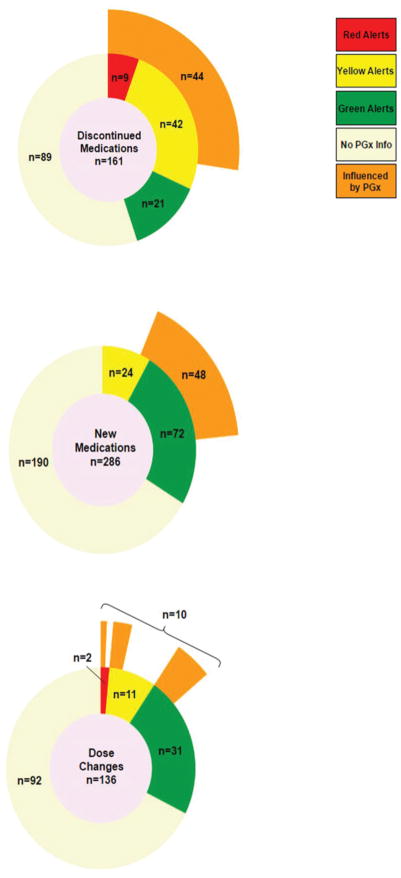
Changes in behavior are necessary to apply genomic discoveries to practice. We prospectively studied medication changes made by providers representing eight different medicine specialty clinics whose patients had submitted to preemptive pharmacogenomic genotyping. An institutional clinical decision support (CDS) system provided pharmacogenomic results using traffic light alerts: green = genomically favorable, yellow = genomic caution, red = high risk. The influence of pharmacogenomic alerts on prescribing behaviors was the primary endpoint. In all, 2,279 outpatient encounters were analyzed. Independent of other potential prescribing mediators, medications with high pharmacogenomic risk were changed significantly more often than prescription drugs lacking pharmacogenomic information (odds ratio (OR) = 26.2 (9.0-75.3), P < 0.0001). Medications with cautionary pharmacogenomic information were also changed more frequently (OR = 2.4 (1.7-3.5), P < 0.0001). No pharmacogenomically high-risk medications were prescribed during the entire study when physicians consulted the CDS tool. Pharmacogenomic information improved prescribing in patterns aimed at reducing patient risk, demonstrating that enhanced prescription decision-making is achievable through clinical integration of genomic medicine.
© 2017 American Society for Clinical Pharmacology and Therapeutics.
Figures
References
-
- Nussbaum RL, McInnes RR, Willard HF, Hamosh A, Thompson MW. Thompson & Thompson genetics in medicine. Philadelphia: Saunders/Elsevier; 2007. Available from: http://site.ebrary.com/lib/uchicago/docDetail.action?docID=10567394.
-
- Spear BB, Heath-Chiozzi M, Huff J. Clinical application of pharmacogenetics. Trends in molecular medicine. 2001;7(5):201–4. - PubMed
-
- Klein TE, Altman RB. PharmGKB: the pharmacogenetics and pharmacogenomics knowledge base. The pharmacogenomics journal. 2004;4(1):1. - PubMed
-
- Altman RB. Pharmacogenomics: “noninferiority” is sufficient for initial implementation. Clinical pharmacology and therapeutics. 2011;89(3):348–50. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
