

Early Systolic Dysfunction Following Traumatic Brain Injury: A Cohort Study
- PMID: 28398926
- PMCID: PMC5433903
- DOI: 10.1097/CCM.0000000000002404
Early Systolic Dysfunction Following Traumatic Brain Injury: A Cohort Study
Abstract
Objective: Prior studies have suggested that traumatic brain injury may affect cardiac function. Our study aims were to determine the frequency, longitudinal course, and admission risk factors for systolic dysfunction in patients with moderate-severe traumatic brain injury.
Design: Prospective cohort study.
Setting: Level 1 trauma center.
Measurements: Transthoracic echocardiogram within 1 day and over the first week after moderate-severe traumatic brain injury; transthoracic echocardiogram within 1 day after mild traumatic brain injury (comparison group).
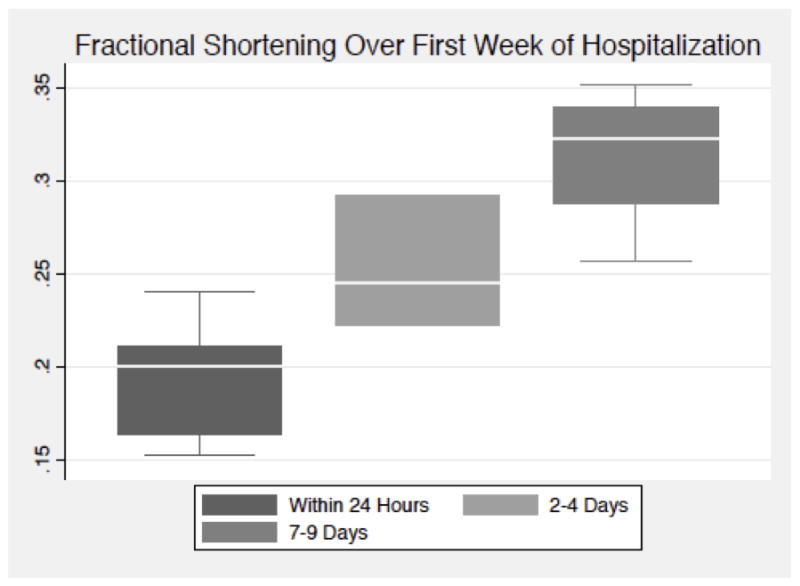
Measurements and main results: Systolic function was assessed by transthoracic echocardiogram, and systolic dysfunction was defined as fractional shortening less than 25%. Multivariable Poisson regression models examined admission risk factors for systolic dysfunction. Systolic function in 32 patients with isolated moderate-severe traumatic brain injury and 32 patients with isolated mild traumatic brain injury (comparison group) was assessed with transthoracic echocardiogram. Seven (22%) moderate-severe traumatic brain injury and 0 (0%) mild traumatic brain injury patients had systolic dysfunction within the first day after injury (p < 0.01). All patients with early systolic dysfunction recovered in 1 week. Younger age (relative risk, 0.87; 95% CI, 0.79-0.94; for 1 yr increase in age) and lower admission Glasgow Coma Scale score (relative risk, 0.34; 95% CI, 0.20-0.58; for one unit increase in Glasgow Coma Scale) were independently associated with the development of systolic dysfunction among moderate-severe traumatic brain injury patients.
Conclusions: Early systolic dysfunction can occur in previously healthy patients with moderate-severe traumatic brain injury, and it is reversible over the first week of hospitalization. Younger age and lower admission Glasgow Coma Scale score are independently associated with the development of systolic dysfunction after moderate-severe traumatic brain injury.
Conflict of interest statement
Conflicts of Interest: None
Figures
Comment in
-
Cardiac Function Following Traumatic Brain Injury.Crit Care Med. 2017 Nov;45(11):e1193-e1194. doi: 10.1097/CCM.0000000000002616. Crit Care Med. 2017. PMID: 29028719 No abstract available.
-
The authors reply.Crit Care Med. 2017 Nov;45(11):e1194-e1195. doi: 10.1097/CCM.0000000000002663. Crit Care Med. 2017. PMID: 29028720 Free PMC article. No abstract available.
-
Systolic Dysfunction Following Traumatic Brain Injury.Crit Care Med. 2018 Feb;46(2):e183. doi: 10.1097/CCM.0000000000002812. Crit Care Med. 2018. PMID: 29337821 No abstract available.
-
The authors reply.Crit Care Med. 2018 Feb;46(2):e183-e184. doi: 10.1097/CCM.0000000000002865. Crit Care Med. 2018. PMID: 29337822 Free PMC article. No abstract available.
References
-
- Rutland-Brown W, Langlois JA, Thomas KE, et al. Incidence of traumatic brain injury in the United States, 2003. J Head Trauma Rehabil. 2006;21(6):544–8. - PubMed
-
- Mascia L, Sakr Y, Pasero D, et al. Extracranial complications in patients with acute brain injury: a post-hoc analysis of the SOAP study. Intensive care medicine. 2008;34(4):720–7. - PubMed
-
- Jeremitsky E, Omert L, Dunham CM, et al. Harbingers of poor outcome the day after severe brain injury: hypothermia, hypoxia, and hypoperfusion. J Trauma. 2003;54(2):312–9. - PubMed
-
- Chesnut RM, Marshall LF, Klauber MR, et al. The role of secondary brain injury in determining outcome from severe head injury. J Trauma. 1993;34(2):216–22. - PubMed
-
- Zafar SN, Millham FH, Chang Y, et al. Presenting blood pressure in traumatic brain injury: a bimodal distribution of death. J Trauma. 2011;71(5):1179–84. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
