

Comparison of surveillance-based metrics for the assessment and monitoring of disease detection: simulation study about type 2 diabetes
- PMID: 28399821
- PMCID: PMC5387346
- DOI: 10.1186/s12874-017-0328-2
Comparison of surveillance-based metrics for the assessment and monitoring of disease detection: simulation study about type 2 diabetes
Abstract
Background: Screening and detection of cases are a common public health priority for treatable chronic conditions with long subclinical periods. However, the validity of commonly-used metrics from surveillance systems for rates of detection (or case-finding) have not been evaluated.
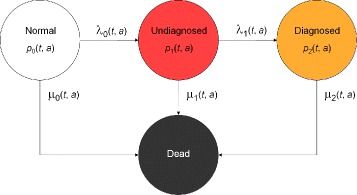
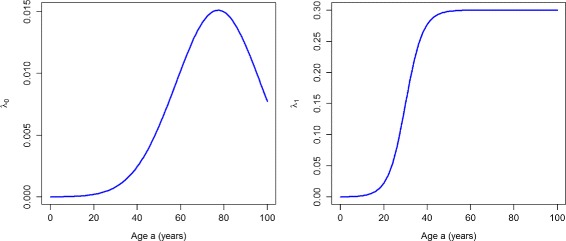
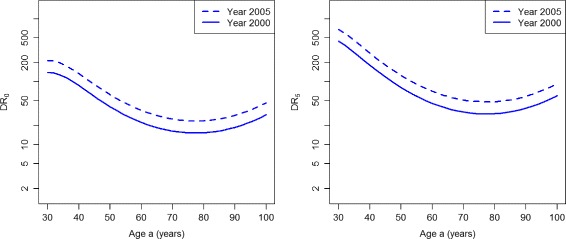
Methods: Using data from a Danish diabetes register and a recently developed illness-death model of chronic diseases with subclinical conditions, we simulate two scenarios of different performance of case-finding. We report different epidemiological indices to assess case-finding in both scenarios and compare the validity of the results.
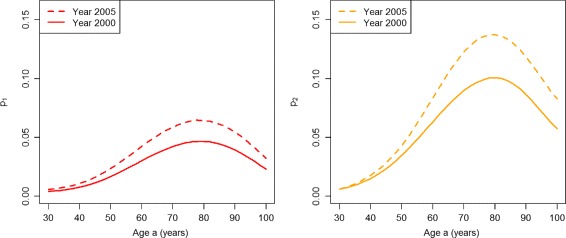
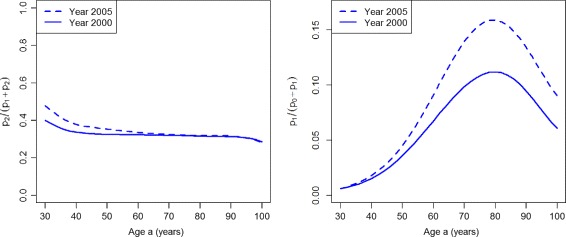
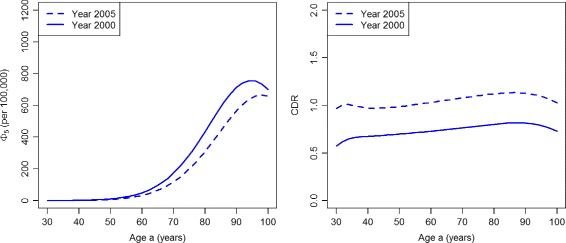
Results: The commonly used ratio of detected cases over total cases may lead to misleading conclusions. Instead, the ratio of undetected cases over persons without a diagnosis is a more valid index to distinguish the quality of case-finding. However, incidence-based measures are preferable to prevalence based indicators.
Conclusion: Prevalence-based indices for assessing case-finding should be interpreted with caution. If possible, incidence-based indices should be preferred.
Keywords: Case-finding; Chronic disease; Compartment model; Diabetes; Incidence; Prevalence; Screening; Undiagnosed disease.
Figures
References
-
- Ayanian JZ, Zaslavsky AM, Weissman JS, Schneider EC, Ginsburg JA. Undiagnosed hypertension and hypercholesterolemia among uninsured and insured adults in the third National Health and Nutrition Examination Survey. Am J Public Health. 2003;93(12):2051–054. doi: 10.2105/AJPH.93.12.2051. - DOI - PMC - PubMed
-
- Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, Adair-Rohani H, AlMazroa MA, Amann M, Anderson HR, Andrews KG, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2013;380(9859):2224–260. doi: 10.1016/S0140-6736(12)61766-8. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
