

Parent Preferences and Perceptions of Milliliters and Teaspoons: Role of Health Literacy and Experience
- PMID: 28400304
- PMCID: PMC5632573
- DOI: 10.1016/j.acap.2017.04.001
Parent Preferences and Perceptions of Milliliters and Teaspoons: Role of Health Literacy and Experience
Abstract
Background and objectives: A recent American Academy of Pediatrics policy statement recommends milliliter-exclusive dosing for pediatric liquid medications. Little is known about parent preferences regarding units, perceptions about moving to milliliters only, and the role of health literacy and prior milliliter-dosing experience.
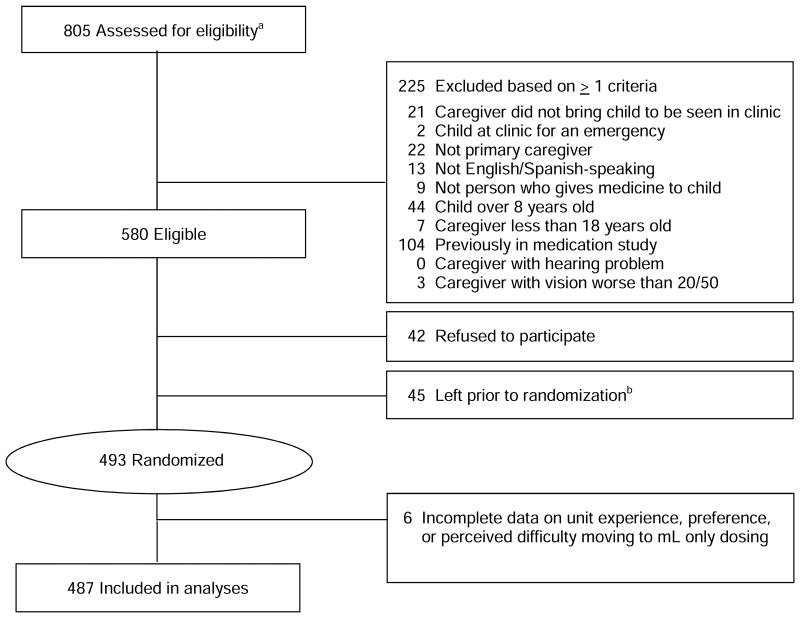
Methods: Cross-sectional analysis of data collected as part of a randomized controlled study in 3 urban pediatric clinics (SAFE Rx for Kids study). English- and Spanish-speaking parents (n = 493) of children aged ≤8 years were randomized to 1 of 4 study arms and given labels and dosing tools which varied in label instruction format (text plus pictogram, text only) and units (milliliter only ["mL"], milliliter/teaspoon ["mL"/"tsp"]). Outcomes included teaspoon preference in dosing instructions and perceived difficulty with milliliter-only dosing. The predictor variable was health literacy (Newest Vital Sign; low [0-1], marginal [2-3], adequate [4-6]). The mediating variable was prior milliliter-dosing experience.
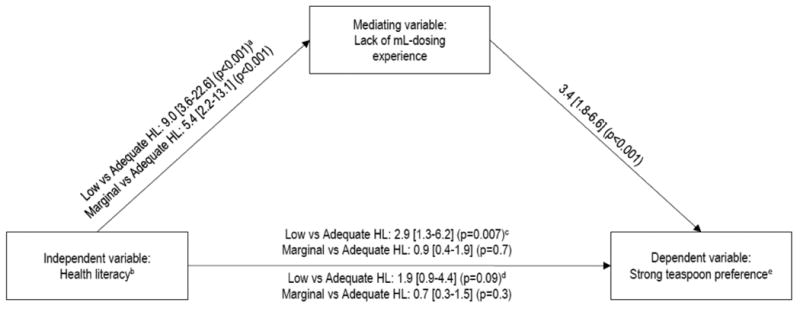
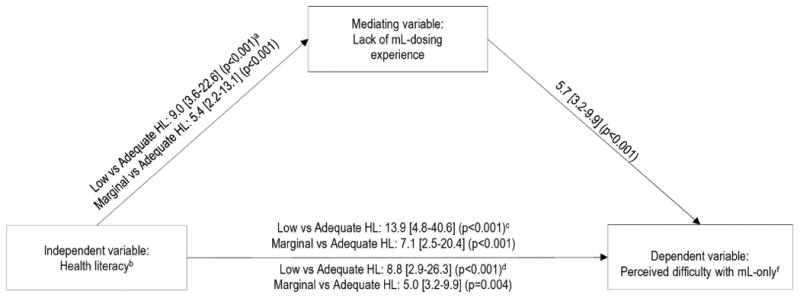
Results: Over two-thirds of parents had low or marginal health literacy. The majority (>70%) preferred to use milliliters, perceived milliliter-only dosing to be easy, and had prior milliliter-dosing experience; 11.5% had a teaspoon preference, 18.1% perceived milliliter-only dosing will be difficult, and 17.7% had no prior milliliter-dosing experience. Parents with lower health literacy had a higher odds of having a teaspoon preference (low vs adequate: adjusted odds ratio [AOR] = 2.9 [95% confidence interval [CI] 1.3-6.2]), and greater odds of perceiving difficulty with milliliter-only dosing (low vs adequate: AOR = 13.9 [95% CI 4.8-40.6], marginal vs adequate: AOR = 7.1 [95% CI 2.5-20.4]). Lack of experience with milliliter dosing partially mediated the impact of health literacy.
Conclusions: Most parents were comfortable with milliliter-only dosing. Parents with low health literacy were more likely to perceive milliliter-only dosing to be difficult; educational efforts will need to target this group to ensure safe medication use.
Keywords: ambulatory care; dosing errors; dosing units; health communication; health literacy; medication errors.
Copyright © 2017 Academic Pediatric Association. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Similar articles
-
Effect of Medication Label Units of Measure on Parent Choice of Dosing Tool: A Randomized Experiment.Acad Pediatr. 2016 Nov-Dec;16(8):734-741. doi: 10.1016/j.acap.2016.04.012. Epub 2016 May 4. Acad Pediatr. 2016. PMID: 27155289 Free PMC article. Clinical Trial.
-
Pictograms, Units and Dosing Tools, and Parent Medication Errors: A Randomized Study.Pediatrics. 2017 Jul;140(1):e20163237. doi: 10.1542/peds.2016-3237. Pediatrics. 2017. PMID: 28759396 Free PMC article. Clinical Trial.
-
Liquid Medication Dosing Errors by Hispanic Parents: Role of Health Literacy and English Proficiency.Acad Pediatr. 2017 May-Jun;17(4):403-410. doi: 10.1016/j.acap.2016.10.001. Acad Pediatr. 2017. PMID: 28477800 Free PMC article.
-
The Relationship of Parental Health Literacy to Health Outcomes of Children with Medical Complexity.J Pediatr Nurs. 2021 Sep-Oct;60:65-70. doi: 10.1016/j.pedn.2021.02.014. Epub 2021 Feb 20. J Pediatr Nurs. 2021. PMID: 33621896 Review.
-
Medicine use in children: a critical area.J Clin Pediatr Dent. 2010 Spring;34(3):207-11. doi: 10.17796/jcpd.34.3.a1w397x29h436tpt. J Clin Pediatr Dent. 2010. PMID: 20578656 Review.
Cited by
-
Primary Care Provider Perceptions and Practices Regarding Dosing Units for Oral Liquid Medications.Acad Pediatr. 2018 May-Jun;18(4):405-408. doi: 10.1016/j.acap.2017.12.002. Epub 2017 Dec 18. Acad Pediatr. 2018. PMID: 29269029 Free PMC article.
-
Changes in Provider Perceptions and Practices Regarding Dosing Units for Oral Liquid Medications.Acad Pediatr. 2024 May-Jun;24(4):627-632. doi: 10.1016/j.acap.2023.08.020. Epub 2023 Sep 4. Acad Pediatr. 2024. PMID: 37666391 Free PMC article.
-
Pharmacotherapy Literacy and Parental Practice in Use of Over-the-Counter Pediatric Medicines.Medicina (Kaunas). 2019 Mar 26;55(3):80. doi: 10.3390/medicina55030080. Medicina (Kaunas). 2019. PMID: 30917624 Free PMC article.
-
Health Literacy-Related Safety Events: A Qualitative Study of Health Literacy Failures in Patient Safety Events.Pediatr Qual Saf. 2021 Jun 23;6(4):e425. doi: 10.1097/pq9.0000000000000425. eCollection 2021 Jul-Aug. Pediatr Qual Saf. 2021. PMID: 34235353 Free PMC article.
-
Syntax Error: Variations in the Verbiage of Prescription Labels for Pediatric Liquid Medications.Cureus. 2024 Mar 12;16(3):e56039. doi: 10.7759/cureus.56039. eCollection 2024 Mar. Cureus. 2024. PMID: 38606237 Free PMC article.
References
-
- National Council for Prescription Drug Programs. NCPDP Recommendations and Guidance for Standardizing the Dosing Designations on Prescription Container Labels of Oral Liquid Medications. NCPDP. 2014 Mar; 2014; White Papers.
-
- Mowry JB, Spyker DA, Brooks DE, Zimmerman A, Schauben JL. 2015 Annual Report of the American Association of Poison Control Centers' National Poison Data System (NPDS): 33rd Annual Report. Clinical Toxicology. 2016;54(10):924–1109. 2016/11/25. - PubMed
-
- Centers for Disease Control and Prevention. The PROTECT Initiative: Advancing Children's Medication Safety. [Accessed 5/27/2016, 2016];2016 http://www.cdc.gov/MedicationSafety/protect/protect_Initiative.html.
-
- Paul IM. Metric Units and the Preferred Dosing of Orally Administered Liquid Medications. Pediatrics. 2015;135(4)
-
- American Academy of Family Physicians. Preferred Unit of Measurement for Liquid Medications. 2011
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
