

Kidney Outcomes and Risk Factors for Nephritis (Flare/ De Novo) in a Multiethnic Cohort of Pregnant Patients with Lupus
- PMID: 28400421
- PMCID: PMC5460714
- DOI: 10.2215/CJN.11431116
Kidney Outcomes and Risk Factors for Nephritis (Flare/ De Novo) in a Multiethnic Cohort of Pregnant Patients with Lupus
Abstract
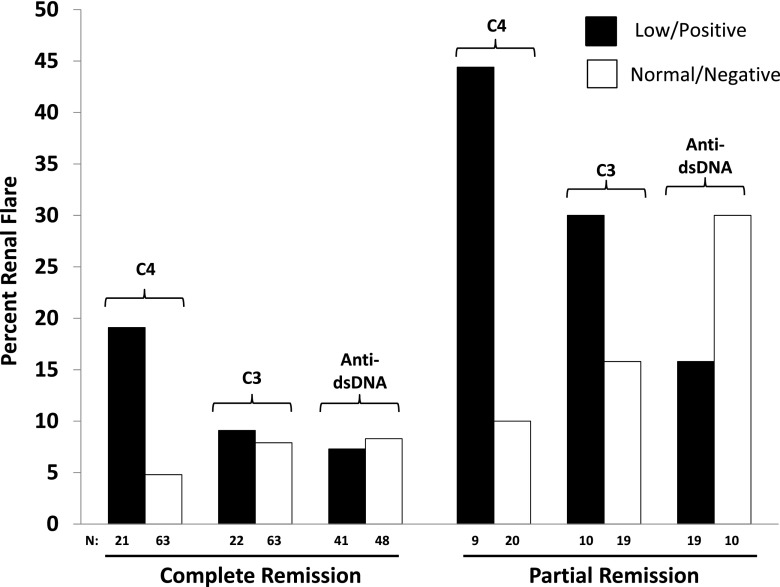
Background and objectives: Kidney disease is a critical concern in counseling patients with lupus considering pregnancy. This study sought to assess the risk of renal flares during pregnancy in women with previous lupus nephritis in partial or complete remission, particularly in those with antidouble-stranded DNA antibodies and low complement levels, and the risk of new-onset nephritis in patients with stable/mildly active SLE.
Design, setting, participants, & measurements: We assessed active nephritis (renal flares and de novo kidney disease) and associated predictors during pregnancy in patients with lupus with urine protein ≤1000 mg and serum creatinine <1.2 mg/dl at baseline; 373 patients (52% ethnic/racial minorities) enrolled between 2003 and 2012 were prospectively followed in the Predictors of Pregnancy Outcome: Biomarkers in Antiphospholipid Syndrome and Systemic Lupus Erythematosus Study. Active nephritis was defined by proteinuria increase of >500 mg and/or red blood cell casts.
Results: Of 118 patients with previous kidney disease, 13 renal flares (11%) occurred (seven of 89 in complete remission and six of 29 in partial remission) compared with four with de novo kidney involvement (2%) in 255 patients without past kidney disease (P<0.001). Active nephritis was not associated with ethnicity, race, age, creatinine, BP, or antihypertensive and other medications. In multivariable logistic regression analyses, patients with past kidney disease in complete or partial remission more often experienced active nephritis (adjusted odds ratio, 6.88; 95% confidence interval, 1.84 to 25.71; P=0.004 and adjusted odds ratio, 20.98; 95% confidence interval, 4.69 to 93.98; P<0.001, respectively) than those without past kidney disease. Low C4 was associated with renal flares/de novo disease (adjusted odds ratio, 5.59; 95% confidence interval, 1.64 to 19.13; P<0.01) but not low C3 or positive anti-dsDNA alone.
Conclusions: De novo kidney involvement in SLE, even in ethnic/racial minorities, is uncommon during pregnancy. Past kidney disease and low C4 at baseline independently associate with higher risk of developing active nephritis. Antibodies to dsDNA alone should not raise concern, even in patients with past kidney disease, if in remission.
Keywords: Antihypertensive Agents; Antiphospholipid Syndrome; Biomarkers; Counseling; Erythrocytes; Female; Humans; Kidney Diseases; Logistic Models; Lupus Erythematosus, Systemic; Pregnancy; Pregnancy Outcome; blood pressure; creatinine; lupus nephritis; proteinuria; risk factors; systemic lupus erythematosus.
Copyright © 2017 by the American Society of Nephrology.
Figures
Similar articles
-
Renal biopsy in the management of lupus nephritis during pregnancy.Lupus. 2015 Feb;24(2):147-54. doi: 10.1177/0961203314551812. Epub 2014 Sep 23. Lupus. 2015. PMID: 25249595
-
Nonrenal and renal activity of systemic lupus erythematosus: a comparison of two anti-C1q and five anti-dsDNA assays and complement C3 and C4.Rheumatol Int. 2012 Aug;32(8):2445-51. doi: 10.1007/s00296-011-1962-3. Epub 2011 Jun 26. Rheumatol Int. 2012. PMID: 21706294
-
Maternal outcome in pregnant women with lupus nephritis. A prospective multicenter study.J Autoimmun. 2016 Nov;74:194-200. doi: 10.1016/j.jaut.2016.06.012. Epub 2016 Jun 30. J Autoimmun. 2016. PMID: 27373903
-
The association between lupus serology and disease outcomes: A systematic literature review to inform the treat-to-target approach in systemic lupus erythematosus.Lupus. 2022 Mar;31(3):307-318. doi: 10.1177/09612033221074580. Epub 2022 Jan 23. Lupus. 2022. PMID: 35067068
-
Pregnancy and lupus nephritis.Scand J Urol Nephrol. 2001 Sep;35(4):319-27. doi: 10.1080/003655901750425927. Scand J Urol Nephrol. 2001. PMID: 11676360 Review.
Cited by
-
What We Do and Do Not Know about Women and Kidney Diseases; Questions Unanswered and Answers Unquestioned: Reflection on World Kidney Day and International Women's Day.Kidney Dis (Basel). 2018 Feb;4(1):37-48. doi: 10.1159/000485269. Epub 2018 Feb 1. Kidney Dis (Basel). 2018. PMID: 29594141 Free PMC article.
-
Immunotherapies application in active stage of systemic lupus erythematosus in pregnancy: A case report and review of literature.World J Clin Cases. 2020 Dec 26;8(24):6396-6407. doi: 10.12998/wjcc.v8.i24.6396. World J Clin Cases. 2020. PMID: 33392323 Free PMC article.
-
Construction and application of fetal loss risk model in systemic lupus erythematosus patients with mild disease severity.BMC Pregnancy Childbirth. 2024 Jul 23;24(1):497. doi: 10.1186/s12884-024-06679-6. BMC Pregnancy Childbirth. 2024. PMID: 39044159 Free PMC article.
-
Predictors Associated with Adverse Pregnancy Outcomes in a Cohort of Women with Systematic Lupus Erythematosus from Romania-An Observational Study (Stage 2).J Clin Med. 2022 Apr 1;11(7):1964. doi: 10.3390/jcm11071964. J Clin Med. 2022. PMID: 35407573 Free PMC article.
-
Lupus nephritis: management challenges during pregnancy.Front Nephrol. 2024 Jun 4;4:1390783. doi: 10.3389/fneph.2024.1390783. eCollection 2024. Front Nephrol. 2024. PMID: 38895665 Free PMC article. Review.
References
-
- Bertsias GK, Tektonidou M, Amoura Z, Aringer M, Bajema I, Berden JHM, Boletis J, Cervera R, Dorner T, Doria A, Ferrario F, Floege J, Houssiau FA, Ioannidis JP, Isenberg DA, Kallenberg CGM, Lightstone L, Marks SD, Martini A, Moroni G, Neumann I, Praga M, Schneider M, Starra A, Tesar V, Vasconcelos C, van Vollenhoven RF, Zakharova H, Haubitz M, Gordon C, Jayne D, Boumpas DT; European League Against Rheumatism and European Renal Association-European Dialysis and Transplant Association : Joint European League Against Rheumatism and European Renal Association-European Dialysis and Transplant Association (EULAR/ERA-EDTA) recommendations for the management of adult and paediatric lupus nephritis. Ann Rheum Dis 71: 1771–1782, 2012 - PMC - PubMed
-
- Linnik MD, Hu JZ, Heilbrunn KR, Strand V, Hurley FL, Joh T; LJP 394 Investigator Consortium : Relationship between anti-double-stranded DNA antibodies and exacerbation of renal disease in patients with systemic lupus erythematosus. Arthritis Rheum 52: 1129–1137, 2005 - PubMed
-
- Saavedra MA, Cruz-Reyes C, Vera-Lastra O, Romero GT, Cruz-Cruz P, Arias-Flores R, Jara LJ: Impact of previous lupus nephritis on maternal and fetal outcomes during pregnancy. Clin Rheumatol 31: 813–819, 2012 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
