

Imaging atherosclerosis in rheumatoid arthritis: evidence for increased prevalence, altered phenotype and a link between systemic and localised plaque inflammation
- PMID: 28400572
- PMCID: PMC5429790
- DOI: 10.1038/s41598-017-00989-w
Imaging atherosclerosis in rheumatoid arthritis: evidence for increased prevalence, altered phenotype and a link between systemic and localised plaque inflammation
Abstract
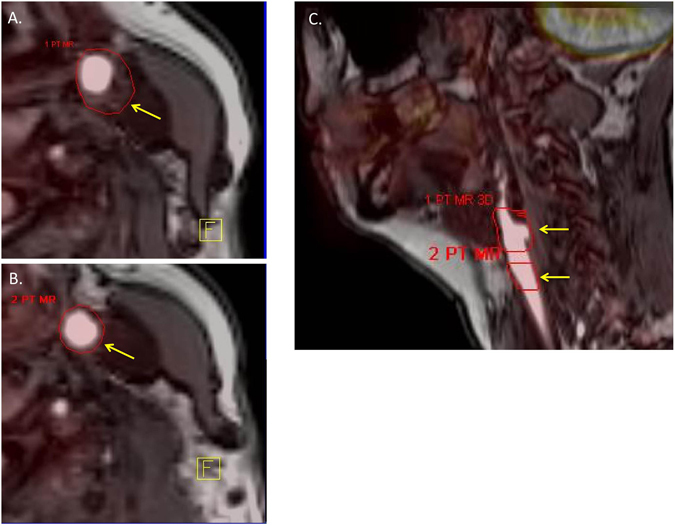
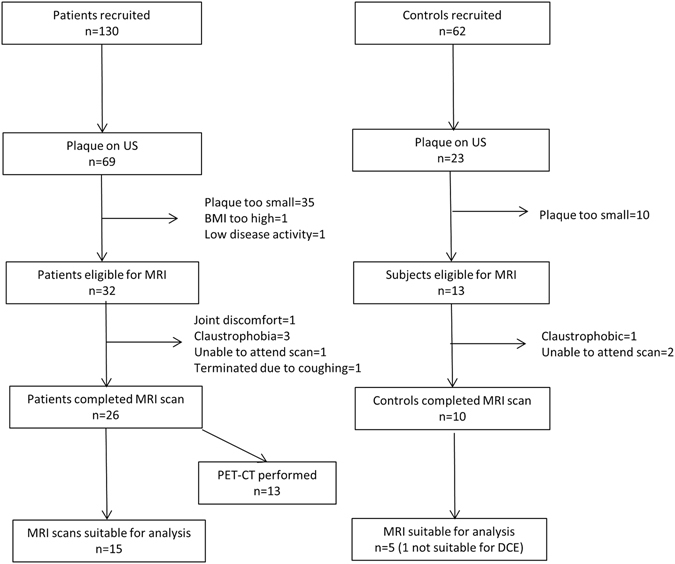
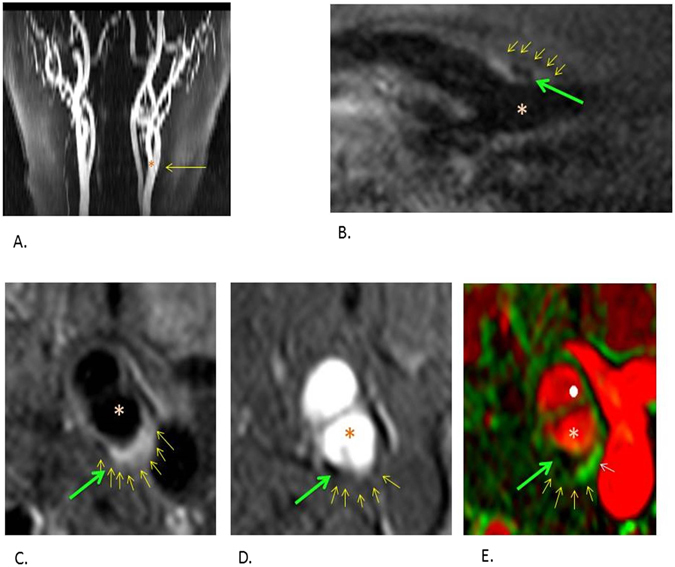
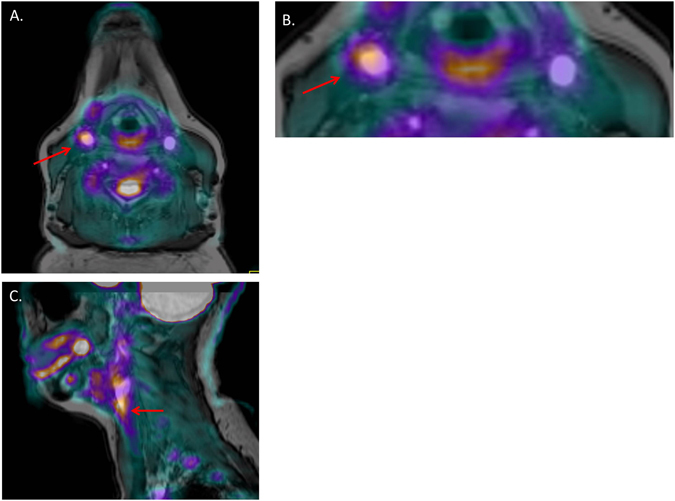
In rheumatoid arthritis (RA), chronic inflammation is thought to drive increased cardiovascular risk through accelerated atherosclerosis. It may also lead to a more high-risk plaque phenotype. We sought to investigate carotid plaque phenotype in RA patients using Dynamic Contrast-Enhanced MRI (DCE-MRI) and Fludeoxyglucose Positron Emission Tomography(FDG-PET). In this pilot study, RA patients and age/sex-matched controls were evaluated for cardiovascular risk factors and carotid plaque on ultrasound. Subjects with plaque >2 mm thick underwent DCE-MRI, and a subgroup of patients had FDG-PET. Comparison of MRI findings between groups and correlation between clinical, serological markers and imaging findings was undertaken. 130 patients and 62 controls were recruited. Plaque was more prevalent in the RA group (53.1% vs 37.0%, p = 0.038) and was independently associated with IL6 levels (HR[95%CI]: 2.03 [1.26, 3.26] per quartile). DCE-MRI data were available in 15 patients and 5 controls. Higher prevalence of plaque calcification was noted in RA, despite similar plaque size (73.3% vs 20%, p = 0.04). FDG-PET detected plaque inflammation in 12/13 patients scanned and degree of inflammation correlated with hs-CRP (r = 0.58, p = 0.04). This study confirms increased prevalence of atherosclerosis in RA and provides data to support the hypothesis that patients have a high-risk plaque phenotype.
Conflict of interest statement
Professor Yuan has received grants from Philips Healthcare and is a board member of Philips Radiology Advisory Board. Professor Hockings reports receiving a salary from Astra Zeneca and Arantos Medical, during the conduct of this study. Professor Waterton has received a salary from Astra Zeneca during the conduct of the study.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
