

Effect of Inpatient Multicomponent Occupational Rehabilitation Versus Less Comprehensive Outpatient Rehabilitation on Sickness Absence in Persons with Musculoskeletal- or Mental Health Disorders: A Randomized Clinical Trial
- PMID: 28401441
- PMCID: PMC5820389
- DOI: 10.1007/s10926-017-9708-z
Effect of Inpatient Multicomponent Occupational Rehabilitation Versus Less Comprehensive Outpatient Rehabilitation on Sickness Absence in Persons with Musculoskeletal- or Mental Health Disorders: A Randomized Clinical Trial
Abstract
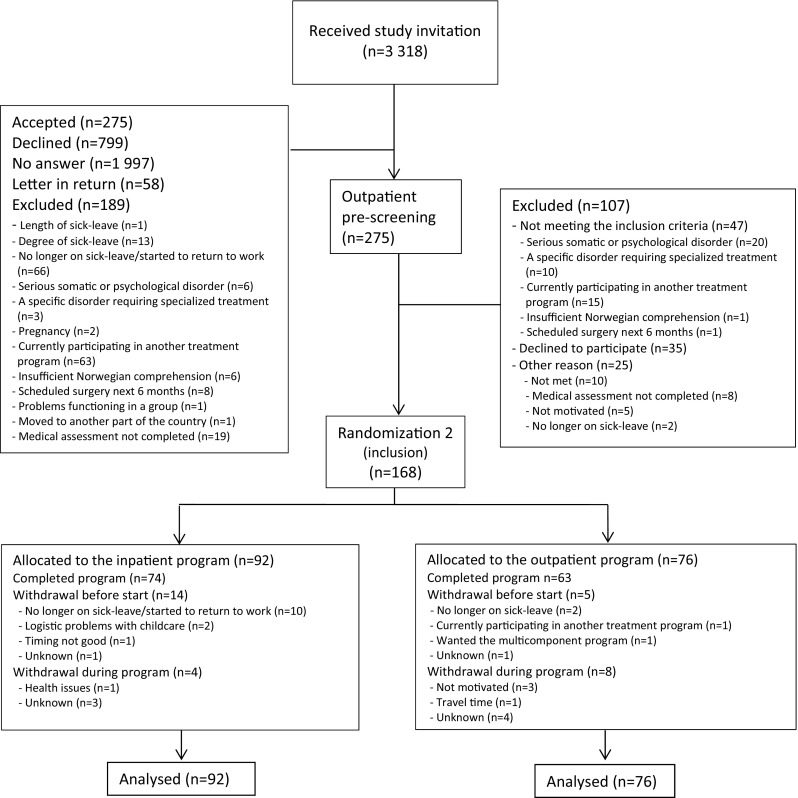
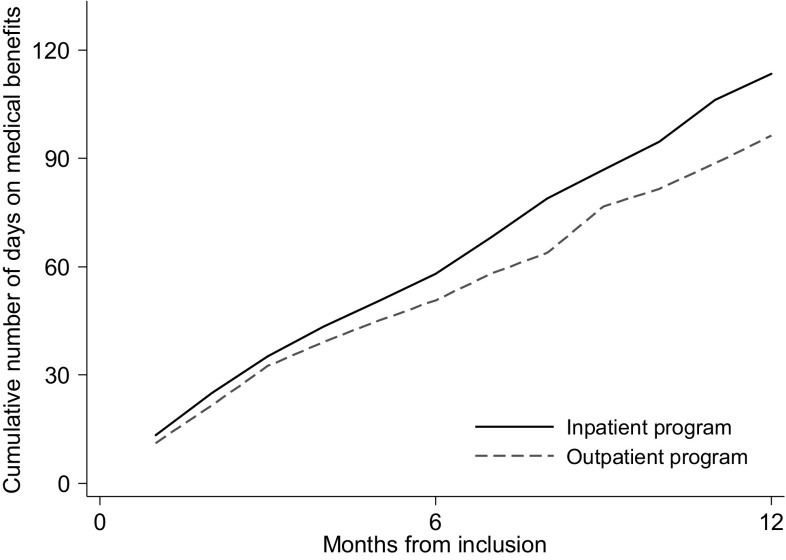
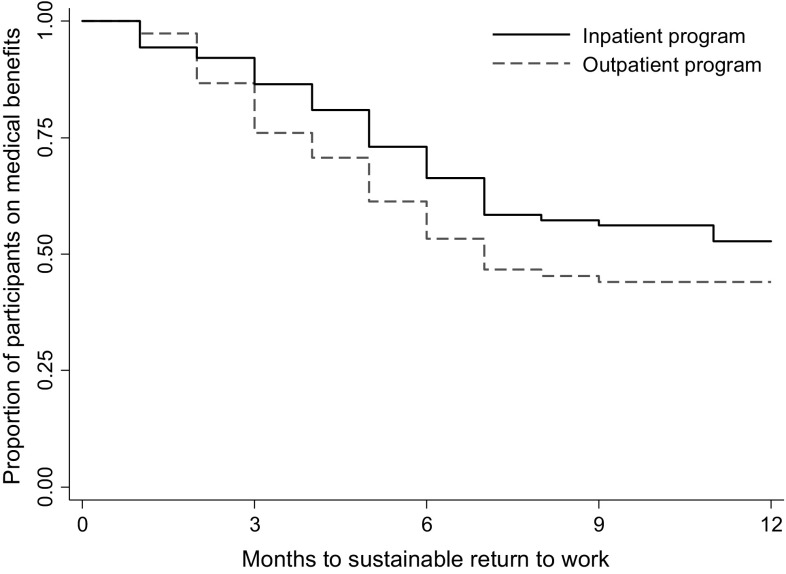
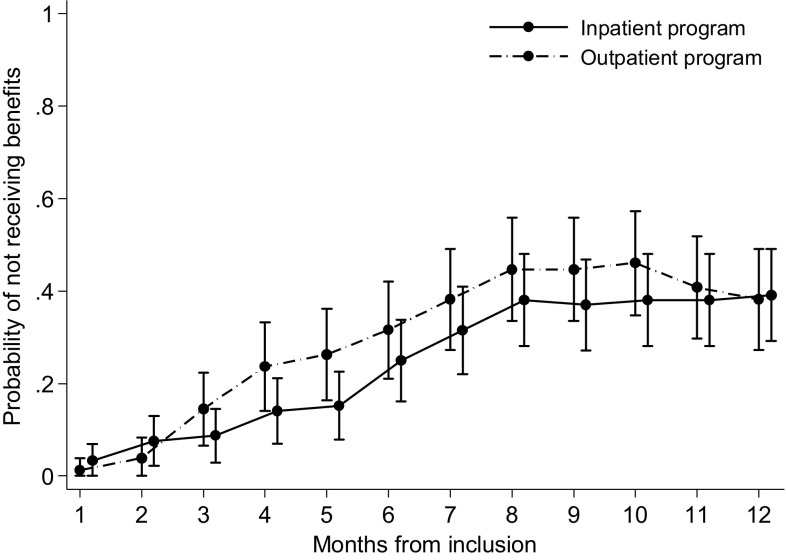
Purpose To assess effects of an inpatient multicomponent occupational rehabilitation program compared to less comprehensive outpatient rehabilitation on sickness absence in persons with musculoskeletal- or mental health disorders. Methods Randomized clinical trial with parallel groups. Participants were individuals 18-60 years old on sick-leave for 2-12 months with a sick-leave diagnosis within the musculoskeletal, psychological or general and unspecified chapters of ICPC-2, identified in a national register. The inpatient program (4 + 4 days) consisted of Acceptance and Commitment Therapy (ACT), physical training and work-related problem-solving including creating a return to work plan and a workplace visit if considered relevant. The outpatient program consisted primarily of ACT (6 sessions during 6 weeks). Both programs were group based. Primary outcome was cumulated number of sickness absence days at 6 and 12 months follow-up. Secondary outcome was time until sustainable return to work. Results 168 individuals were randomized to the inpatient program (n = 92) or the outpatient program (n = 76). We found no statistically significant difference between the programs in median number of sickness absence days at 6 and 12 months follow-up. In the outpatient program 57% of the participants achieved sustainable return to work (median time 7 months), in the inpatient program 49% (log rank, p = 0.167). The hazard ratio for sustainable return to work was 0.74 (95% CI 0.48-1.32, p = 0.165), in favor of the outpatient program. Conclusions This study provided no support that the more comprehensive 4 + 4 days inpatient multicomponent occupational rehabilitation program reduced sickness absence compared to the outpatient rehabilitation program.
Keywords: Cognitive therapy; Mental health; Musculoskeletal diseases; Return to work; Sick leave.
Conflict of interest statement
Conflict of interest
Marius Steiro Fimland was previously employed at Hysnes Rehabilitation Center, St. Olavs Hospital, and is currently employed at Department of Physical Medicine and Rehabilitation, St. Olavs Hospital. Sigmund Gismervik is employed at Department of Physical Medicine and Rehabilitation, St. Olavs Hospital. The other authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Figures
References
-
- OECD . Sickness, disability and work: breaking the barriers. Paris: OECD Publishing; 2010.
-
- OECD . Mental health and work. Paris: OECD Publishing; 2013.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
