

Deep Phenotyping of Systemic Arterial Hemodynamics in HFpEF (Part 2): Clinical and Therapeutic Considerations
- PMID: 28401511
- PMCID: PMC5515667
- DOI: 10.1007/s12265-017-9736-2
Deep Phenotyping of Systemic Arterial Hemodynamics in HFpEF (Part 2): Clinical and Therapeutic Considerations
Abstract
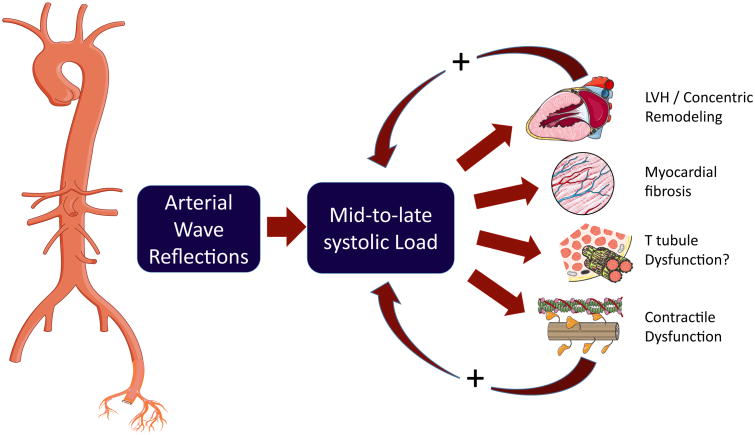
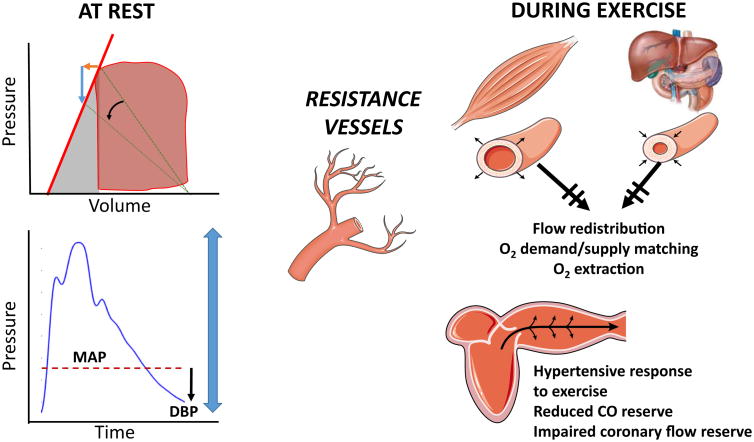
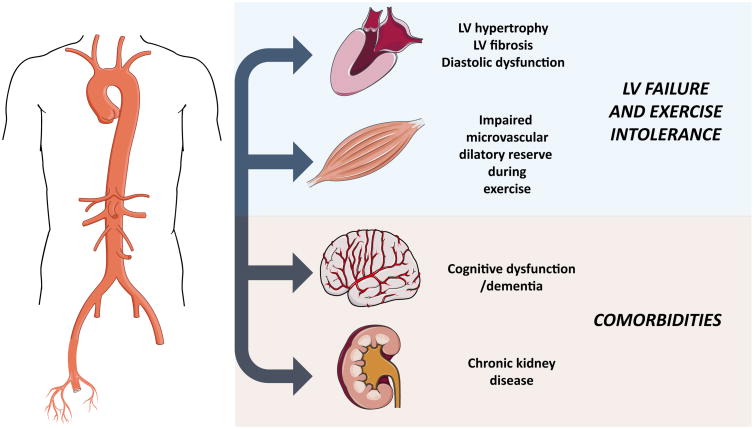
Multiple phase III trials over the last few decades have failed to demonstrate a clear benefit of various pharmacologic interventions in heart failure with a preserved left ventricular (LV) ejection fraction (HFpEF). Therefore, a better understanding of its pathophysiology is important. An accompanying review describes key technical and physiologic aspects regarding the deep phenotyping of arterial hemodynamics in HFpEF. This review deals with the potential of this approach to enhance our clinical, translational, and therapeutic approach to HFpEF. Specifically, the role of arterial hemodynamics is discussed in relation to (1) the pathophysiology of left ventricular diastolic dysfunction, remodeling, and fibrosis, (2) impaired oxygen delivery to peripheral skeletal muscle, which affects peripheral oxygen extraction, (3) the frequent presence of comorbidities, such as renal failure and dementia in this population, and (4) the potential to enhance precision medicine approaches. A therapeutic approach to target arterial hemodynamic abnormalities that are prevalent in this population (particularly, with inorganic nitrate/nitrite) is also discussed.
Keywords: Afterload; Arterial hemodynamics; Comorbidities; Dementia; Exercise intolerance; Heart failure with preserved ejection fraction; Pulsatile load; Renal disease; Wave reflections.
Figures
References
-
- Lloyd-Jones DM, Hong Y, Labarthe D, Mozaffarian D, Appel LJ, Van Horn L, Greenlund K, Daniels S, Nichol G, Tomaselli GF, Arnett DK, Fonarow GC, Ho PM, Lauer MS, Masoudi FA, Robertson RM, Roger V, Schwamm LH, Sorlie P, Yancy CW, Rosamond WD. Defining and setting national goals for cardiovascular health promotion and disease reduction: the American Heart Association's strategic Impact Goal through 2020 and beyond. Circulation. 2010;121:586–613. - PubMed
-
- Townsend RR, Wilkinson IB, Schiffrin EL, Avolio AP, Chirinos JA, Cockcroft JR, Heffernan KS, Lakatta EG, McEniery CM, Mitchell GF, Najjar SS, Nichols WW, Urbina EM, Weber T American Heart Association Council on H. Recommendations for improving and standardizing vascular research on arterial stiffness: a scientific statement from the American Heart Association. Hypertension. 2015;66:698–722. - PMC - PubMed
-
- Hoekstra T, Lesman-Leegte I, van Veldhuisen DJ, Sanderman R, Jaarsma T. Quality of life is impaired similarly in heart failure patients with preserved and reduced ejection fraction. European Journal of Heart Failure. 2011;13:1013–1018. - PubMed
-
- Lewis EF, Lamas GA, O'Meara E, Granger CB, Dunlap ME, McKelvie RS, Probstfield JL, Young JB, Michelson EL, Halling K, Carlsson J, Olofsson B, McMurray JJ, Yusuf S, Swedberg K, Pfeffer MA. Characterization of health-related quality of life in heart failure patients with preserved versus low ejection fraction in CHARM. European Journal of Heart Failure. 2007;9:83–91. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
