

Surgical Performance in Minimally Invasive Surgery Plus Recombinant Tissue Plasminogen Activator for Intracerebral Hemorrhage Evacuation Phase III Clinical Trial
- PMID: 28402516
- PMCID: PMC6257031
- DOI: 10.1093/neuros/nyx123
Surgical Performance in Minimally Invasive Surgery Plus Recombinant Tissue Plasminogen Activator for Intracerebral Hemorrhage Evacuation Phase III Clinical Trial
Abstract
Background: Minimally invasive thrombolytic evacuation of intracerebral hematoma is being investigated in the ongoing phase III clinical trial of Minimally Invasive Surgery plus recombinant Tissue plasminogen activator for Intracerebral hemorrhage Evacuation (MISTIE III).
Objective: To assess the accuracy of catheter placement and efficacy of hematoma evacuation in relation to surgical approach and surgeon experience.
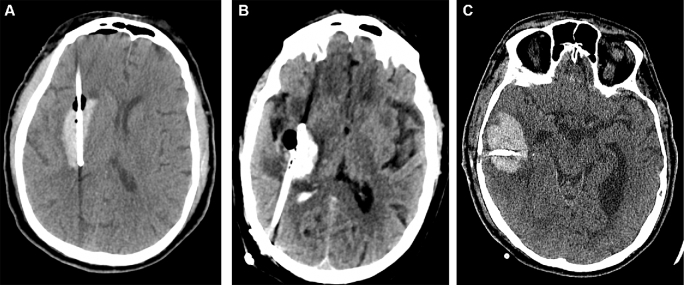
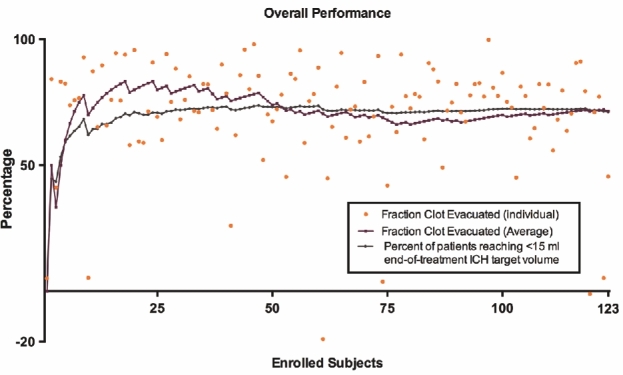
Methods: We performed a trial midpoint interim assessment of 123 cases that underwent the surgical procedure. Accuracy of catheter placement was prospectively assessed by the trial Surgical Center based on prearticulated criteria. Hematoma evacuation efficacy was evaluated based on absolute volume reduction, percentage hematoma evacuation, and reaching the target end-of-treatment volume of <15 mL. One of 3 surgical trajectories was used: anterior (A), posterior (B), and lobar (C). Surgeons were classified based on experience with the MISTIE procedure as prequalified, qualified with probation, and fully qualified.
Results: The average hematoma volume was 49.7 mL (range 20.0-124), and the mean evacuation rate was 71% (range 18.4%-99.8%). First placed catheters were 58% in good position, 28% suboptimal (but suitable to dose), and 14% poor (requiring repositioning). Posterior trajectory (B) was associated with significantly higher rates of poor placement (35%, P = .01). There was no significant difference in catheter placement accuracy among surgeons of varying experience. Hematoma evacuation efficacy was not significantly different among the 3 surgical approaches or different surgeons' experience.
Conclusion: Ongoing surgical education and quality monitoring in MISTIE III have resulted in consistent rates of hematoma evacuation despite technical challenges with the surgical approaches and among surgeons of varying experience.
Keywords: Alteplase; Intracerebral hemorrhage; MISTIE; Minimally invasive; Tissue plasminogen activator.
Copyright © 2017 by the Congress of Neurological Surgeons
Figures
References
-
- Mendelow AD, Gregson BA, Fernandes HM et al. . Early surgery versus initial conservative treatment in patients with spontaneous supratentorial intracerebral haematomas in the International Surgical Trial in Intracerebral Haemorrhage (STICH): a randomised trial. Lancet. 2005;365(9457):387-397. - PubMed
-
- Morgenstern LB, Demchuk AM, Kim DH, Frankowski RF, Grotta JC. Rebleeding leads to poor outcome in ultra-early craniotomy for intracerebral hemorrhage. Neurology. 2001;56(10):1294-1299. - PubMed
-
- Zuccarello M, Brott T, Derex L et al. . Early surgical treatment for supratentorial intracerebral hemorrhage: a randomized feasibility study. Stroke. 1999;30(9):1833-1839. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
