

Effectiveness of Manual Therapy and Stretching for Baseball Players With Shoulder Range of Motion Deficits
- PMID: 28402756
- PMCID: PMC5435155
- DOI: 10.1177/1941738117702835
Effectiveness of Manual Therapy and Stretching for Baseball Players With Shoulder Range of Motion Deficits
Abstract
Background: Baseball players displaying deficits in shoulder range of motion (ROM) are at increased risk of arm injury. Currently, there is a lack of consensus regarding the best available treatment options to restore shoulder ROM.
Hypothesis: Instrumented manual therapy with self-stretching will result in clinically significant deficit reductions when compared with self-stretching alone.
Study design: Controlled laboratory study.
Methods: Shoulder ROM and humeral torsion were assessed in 60 active baseball players (mean age, 19 ± 2 years) with ROM deficits (nondominant - dominant, ≥15°). Athletes were randomly assigned to receive a single treatment of instrumented manual therapy plus self-stretching (n = 30) or self-stretching only (n = 30). Deficits in internal rotation, horizontal adduction, and total arc of motion were compared between groups immediately before and after a single treatment session. Treatment effectiveness was determined by mean comparison data, and a number-needed-to-treat (NNT) analysis was used for assessing the presence of ROM risk factors.
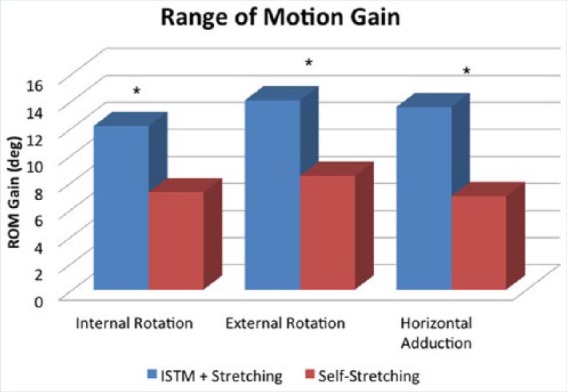
Results: Prior to intervention, players displayed significant ( P < 0.001) dominant-sided deficits in internal rotation (-26°), total arc of motion (-18°), and horizontal adduction (-17°). After the intervention, both groups displayed significant improvements in ROM, with the instrumented manual therapy plus self-stretching group displaying greater increases in internal rotation (+5°, P = 0.010), total arc of motion (+6°, P = 0.010), and horizontal adduction (+7°, P = 0.004) compared with self-stretching alone. For horizontal adduction deficits, the added use of instrumented manual therapy with self-stretching decreased the NNT to 2.2 (95% CI, 2.1-2.4; P = 0.010).
Conclusion: Instrumented manual therapy with self-stretching significantly reduces ROM risk factors in baseball players with motion deficits when compared with stretching alone.
Clinical relevance: The added benefits of manual therapy may help to reduce ROM deficits in clinical scenarios where stretching alone is ineffective.
Keywords: baseball; glenohumeral internal rotation deficit (GIRD); instrumented manual therapy; posterior shoulder tightness (PST).
Conflict of interest statement
The authors report no potential conflicts of interest in the development and publication of this article.
Figures



References
-
- Awan R, Boon AJ, Smith J. Measuring shoulder internal rotation range of motion: a comparison of 3 techniques. Arch Phys Med Rehabil. 2002;83:1229-1234. - PubMed
-
- Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: spectrum of pathology. Part I: pathoanatomy and biomechanics. Arthroscopy. 2003;19:404-420. - PubMed
-
- Crockett HC, Gross LB, Wilk KE, et al. Osseous adaptation and range of motion at the glenohumeral joint in professional baseball pitchers. Am J Sports Med. 2002;30:20-26. - PubMed
-
- Donatelli R, Ellenbecker TS, Ekedahl SR, Wilkes JS, Kocher K, Adam J. Assessment of shoulder strength in professional baseball pitchers. J Orthop Sports Phys Ther. 2000;30:544-551. - PubMed
-
- Ellenbecker TS, Roetert EP, Bailie DS, Davies GJ, Brown SW. Glenohumeral joint total rotation range of motion in elite tennis players and baseball pitchers. Med Sci Sports Exerc. 2002;34:2052-2056. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
