

Can Vertical Integration Reduce Hospital Readmissions? A Difference-in-Differences Approach
- PMID: 28403012
- PMCID: PMC5398905
- DOI: 10.1097/MLR.0000000000000704
Can Vertical Integration Reduce Hospital Readmissions? A Difference-in-Differences Approach
Abstract
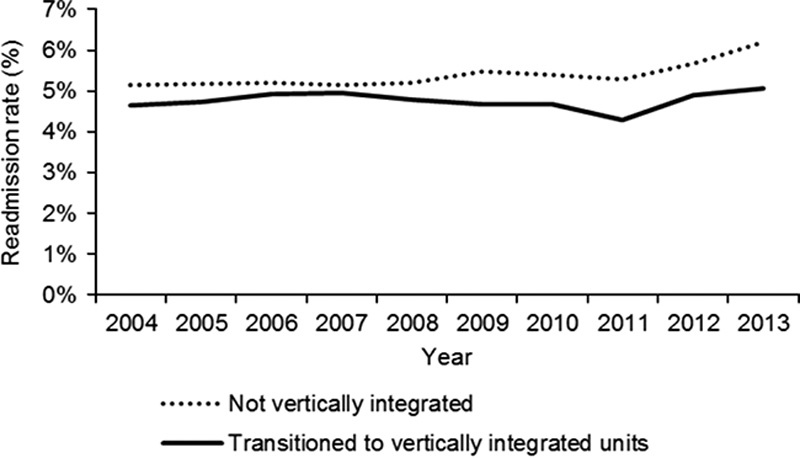
Background: Vertical integration is expected to improve communication and coordination between inpatient care and care after discharge. Despite being used across health systems worldwide, evidence about its impact on readmissions is sparse and contradictory.
Objective: To assess the impact of vertical integration on hospital readmissions.
Research design, subjects, and measures: Using difference-in-differences we compared readmissions before and after vertical integration in 6 Portuguese hospitals for years 2004-2013. A control group with 6 similar hospitals not integrated was utilized. Considered outcome was 30-day unplanned readmission. We used logistic regression at the admission level and accounted for patients' risk factors using claims data. Analyses for each hospital and selected conditions were also run.
Results: Our results suggest that readmissions decreased overall after vertical integration [odds ratio (OR)=0.900; 95% confidence interval (CI), 0.812-0.997]. Hospital analysis indicated that there was no impact for 2 hospitals (OR=0.960; 95% CI, 0.848-1.087 and OR=0.944; 95% CI, 0.857-1.038), and a positive effect in 4 hospitals (greatest effect: OR=0.811; 95% CI, 0.736-0.894). A positive evolution was observed for a limited number of conditions, with better results for diabetes with complications (OR=0.689; 95% CI, 0.525-0.904), but no impact regarding congestive heart failure (OR=1.067; 95% CI, 0.827-1.377).
Conclusions: Merging acute and primary care providers was associated with reduced readmissions, even though improvements were not found for all institutions or condition-specific groups. There are still challenges to be addressed regarding the success of vertical integration in reducing 30-day hospital readmissions.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- World Health Organization. People-Centred and Integrated Health Services: An Overview of the Evidence: Interim Report. Geneva: WHO—World Health Organization; 2015.
-
- Centers for Medicare and Medicaid Services. Improving Quality of Care for Medicare Patients: Accountable Care Organizations. Baltimore, MD: Centers for Medicare and Medicaid Services; 2016.
-
- Shaw S, Rosen R, Rumbold B. An Overview of Integrated Care in the NHS: What is Integrated Care?. London: Nuffield Trust; 2011.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
