

Gabapentin can decrease acute pain and morphine consumption in spinal surgery patients: A meta-analysis of randomized controlled trials
- PMID: 28403075
- PMCID: PMC5403072
- DOI: 10.1097/MD.0000000000006463
Gabapentin can decrease acute pain and morphine consumption in spinal surgery patients: A meta-analysis of randomized controlled trials
Abstract
Background: Approximately 80% of patients who underwent spinal surgeries experience moderate to extreme postoperative pain. Gabapentin was used as an adjunct for the management of acute pain in approximately half of enhanced recovery programs. This meta-analysis aimed to illustrate the efficacy and safety of gabapentin for pain management following spinal surgery.
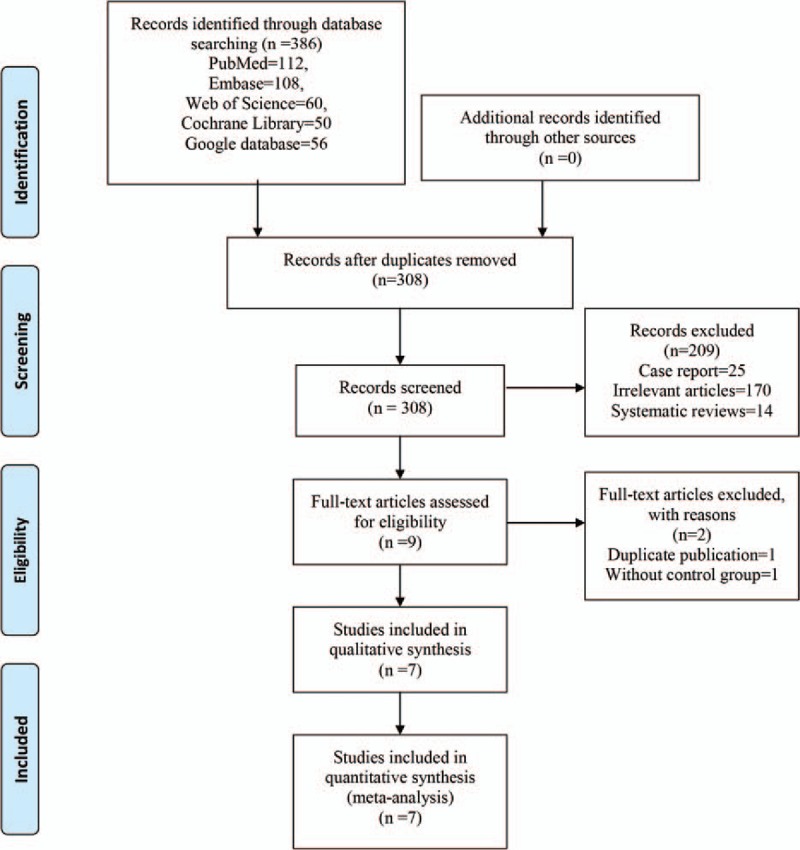
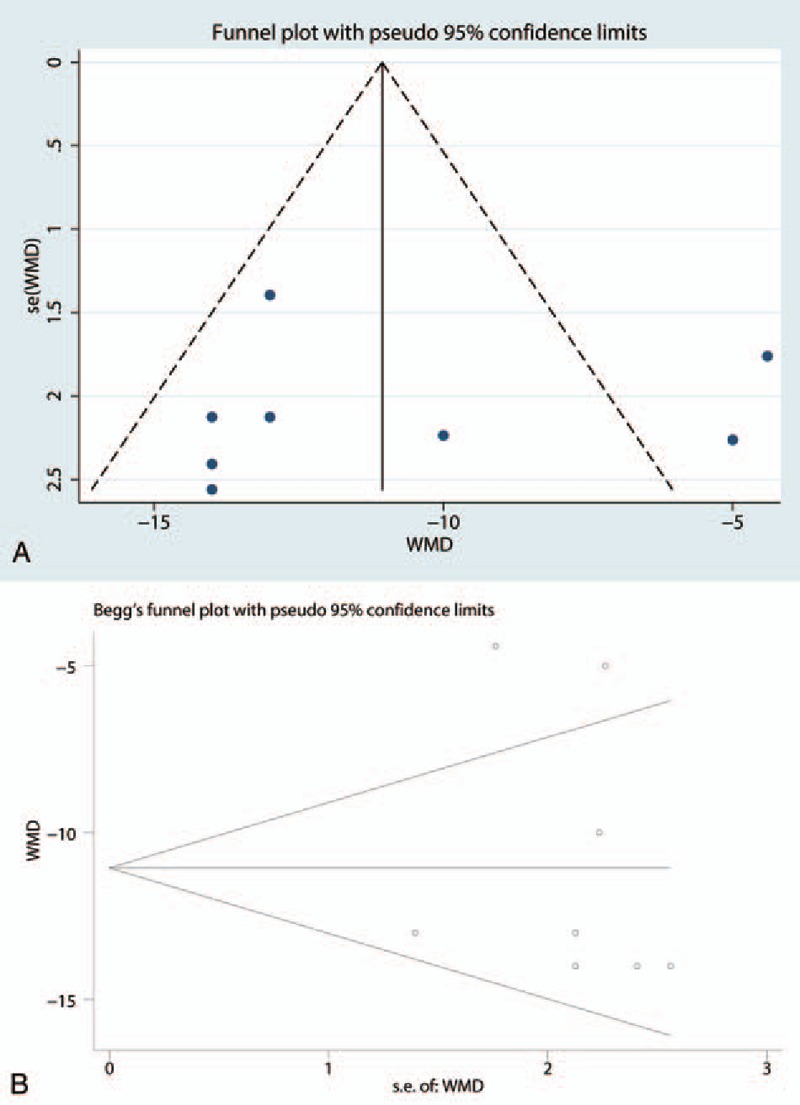
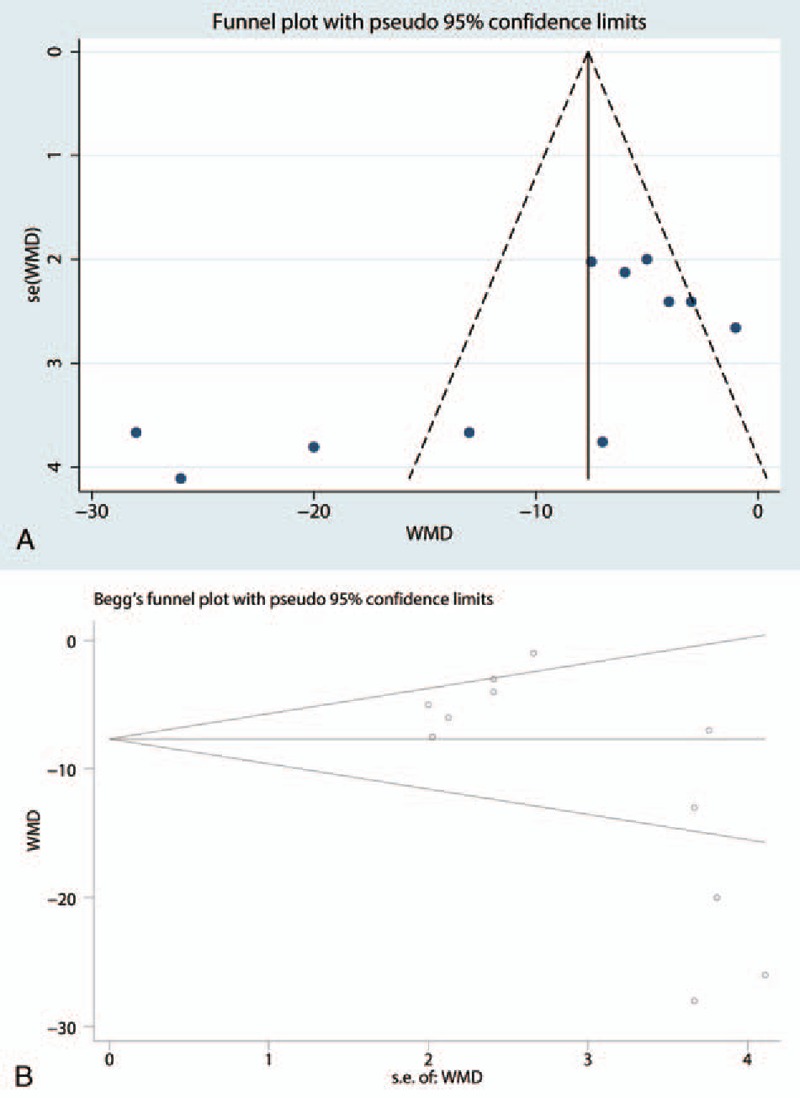
Methods: In January 2017, a systematic computer-based search was conducted in PubMed, EMBASE, Web of Science, Cochrane Database of Systematic Reviews, and Google database. Data on patients prepared for spine surgery in studies that compared gabapentin versus placebo were retrieved. The primary endpoint was the visual analog scale (VAS) at 12 hours and 24 hours and total morphine consumption. The secondary outcomes were complications that included nausea, dizziness, somnolence, headache, pruritus, urine retention, and vomiting. After testing for publication bias and heterogeneity between studies, data were aggregated for random-effects models when necessary.
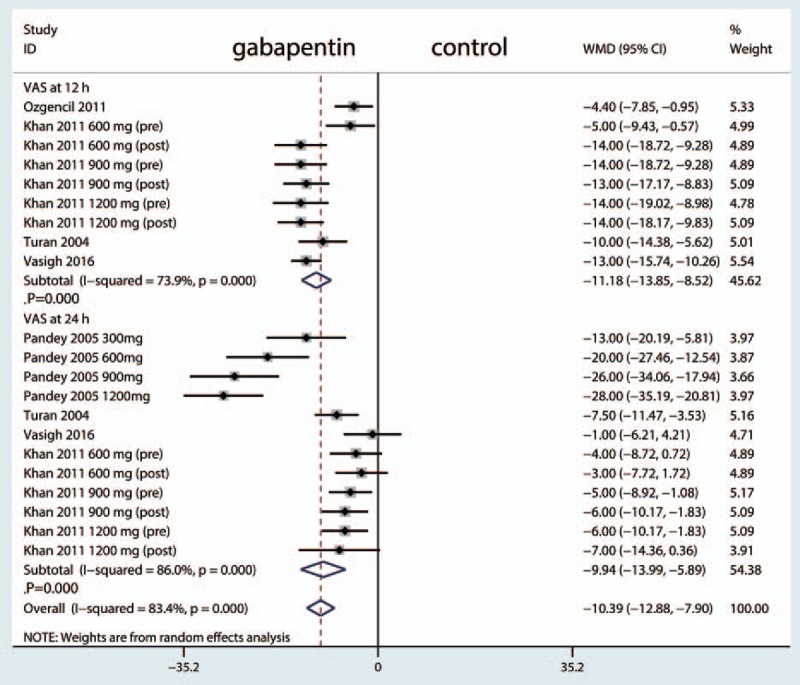
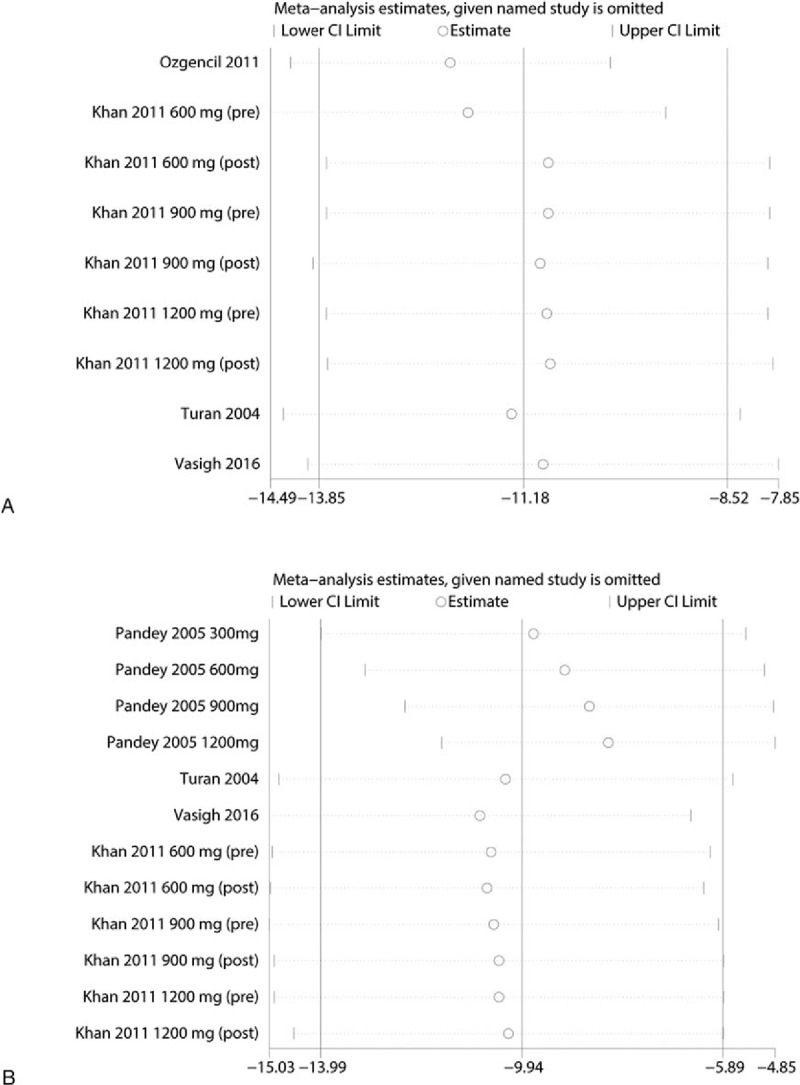
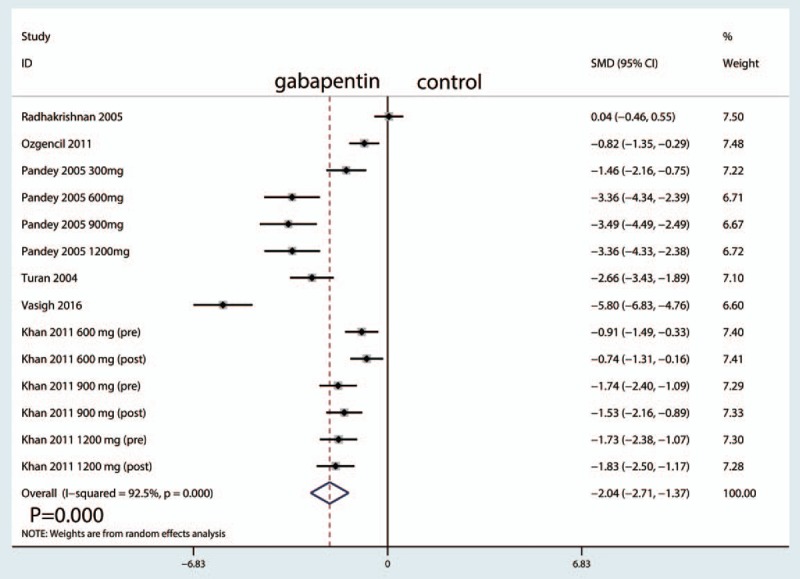
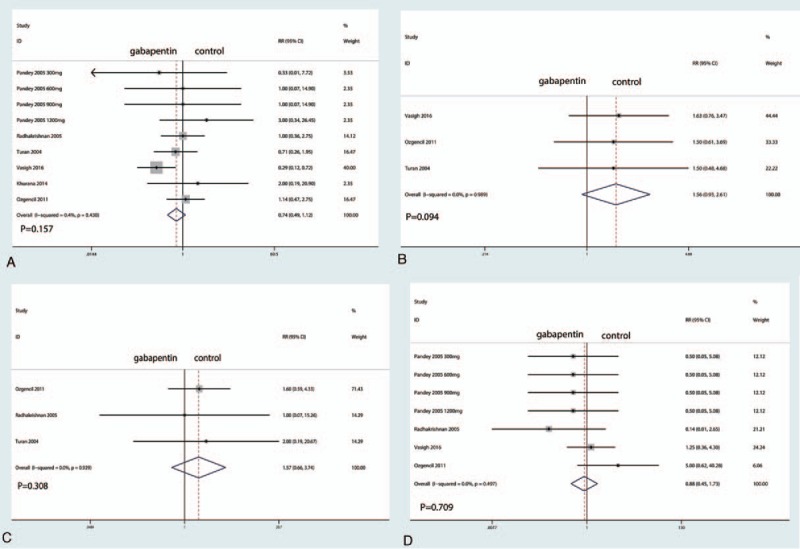
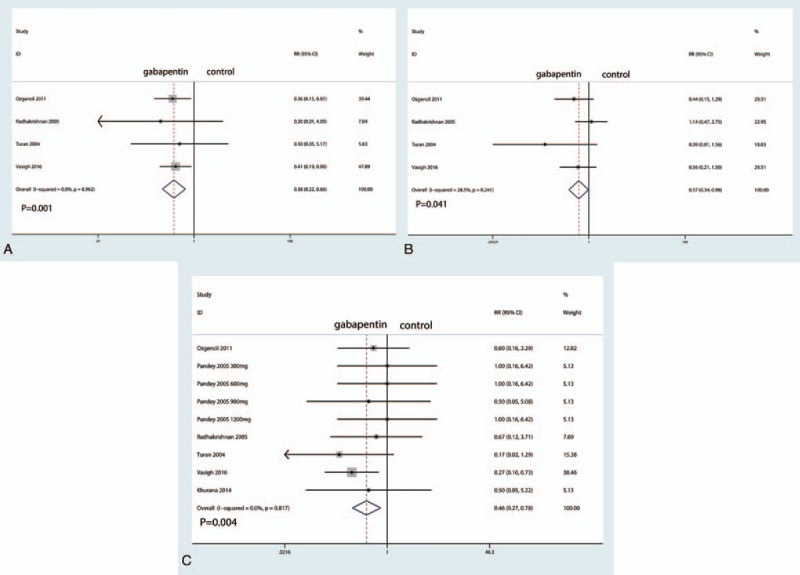
Results: Seven clinical studies with 581 patients (gabapentin group=383, control group=198) were ultimately included in the meta-analysis. Gabapentin was associated with reduced pain scores at 12 hours and 24 hours, corresponding to a reduction of 11.18 points (95% CI, -13.85 to -8.52 points) at 12 hours and 9.94 points (95% CI, -13.99 to -5.89 points) at 24 hours on a 100-point VAS. Similarly, gabapentin was associated with a reduction in total morphine consumption (-2.04, 95% CI -2.71, -1.37). Furthermore, gabapentin can reduce the occurrence of vomiting (risk ratio [RR] 0.46, 95% CI 0.27, 0.78, P = 0.004), urine retention (RR = 0.57, 95% CI 0.34, 0.98, P = 0.041, NNT = 11.9) and pruritus (RR = 0.38, 95% CI 0.22, 0.66, P = 0.001, NNT = 5.6) and the number needed to treat (NNT = 20.1). There were no significant differences in the occurrence of nausea, dizziness, somnolence, or headache.
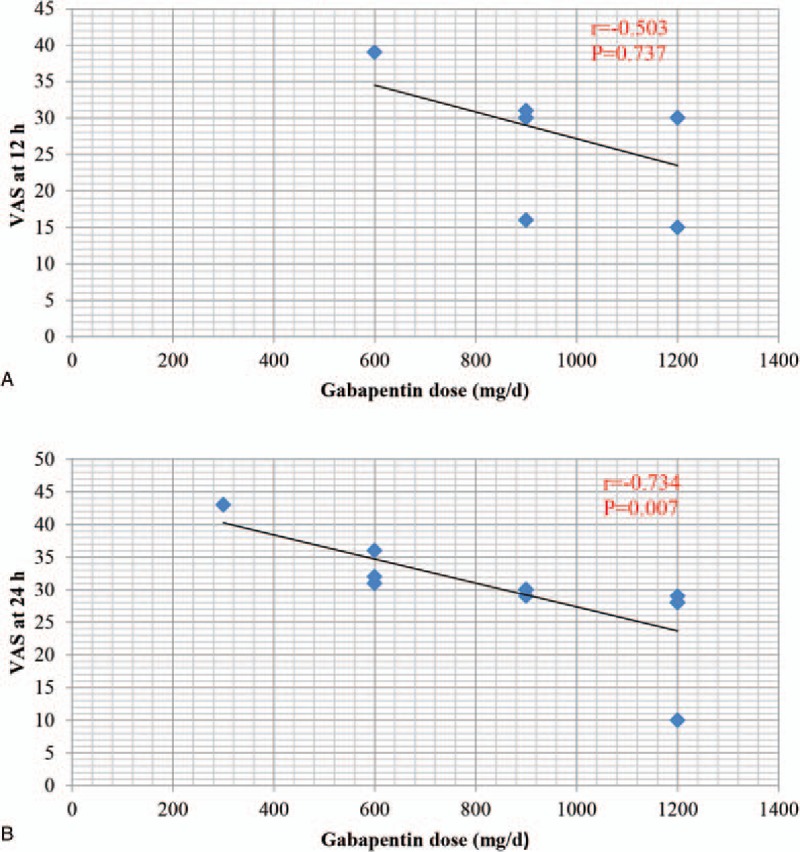
Conclusions: Gabapentin was efficacious in the reduction of postoperative pain, total morphine consumption, and morphine-related complications following spine surgery. In addition, a high dose (≥900 mg/d) of gabapentin is more effective than a low dose (<900 mg/d). The number of included studies is limited, and more studies are needed to verify the effects of gabapentin in spinal surgery patients.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
References
-
- Apfelbaum JL, Chen C, Mehta SS, et al. Postoperative pain experience: results from a national survey suggest postoperative pain continues to be undermanaged. Anesth Analg 2003;97:534–40. table of contents. - PubMed
-
- Ravindran D. Chronic postsurgical pain: prevention and management. J Pain Palliat Care Pharmacother 2014;28:51–3. - PubMed
-
- Dong J, Li W, Wang Y. The effect of pregabalin on acute postoperative pain in patients undergoing total knee arthroplasty: a meta-analysis. Int J Surg 2016;34:148–60. - PubMed
-
- Radhakrishnan M, Bithal PK, Chaturvedi A. Effect of preemptive gabapentin on postoperative pain relief and morphine consumption following lumbar laminectomy and discectomy: a randomized, double-blinded, placebo-controlled study. J Neurosurg Anesthesiol 2005;17:125–8. - PubMed
-
- Dolin SJ, Cashman JN. Tolerability of acute postoperative pain management: nausea, vomiting, sedation, pruritus, and urinary retention. Evidence from published data. Br J Anaesth 2005;95:584–91. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
