

Association of vitamin D deficiency, season of the year, and latent tuberculosis infection among household contacts
- PMID: 28403225
- PMCID: PMC5389794
- DOI: 10.1371/journal.pone.0175400
Association of vitamin D deficiency, season of the year, and latent tuberculosis infection among household contacts
Abstract
Objectives: Vitamin D (VD) enhances the immune response against Mycobacterium tuberculosis in vitro, and VD deficiency has been described in patients with active tuberculosis (TB). However, the role of hypovitaminosis D in the pathogenesis of early TB infection acquisition is unclear. We aimed to evaluate the association of VD deficiency, season of the year, and latent TB infection in household contacts (HHC), given that this is a potentially modifiable condition often related to nutritional deficiencies and lack of sun exposure.
Methods: We prospectively enrolled new pulmonary TB cases (n = 107) and their HHC (n = 144) over a 2-year period in Santiago, Chile. We compared plasma 25-hydroxycholecalciferol (25OHD) levels and examined the influence of season, ethnic background, living conditions, and country of origin.
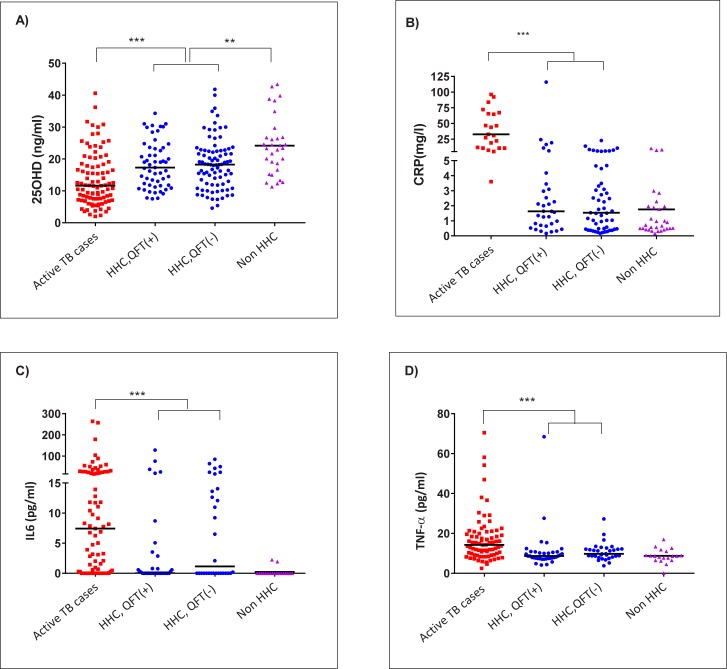
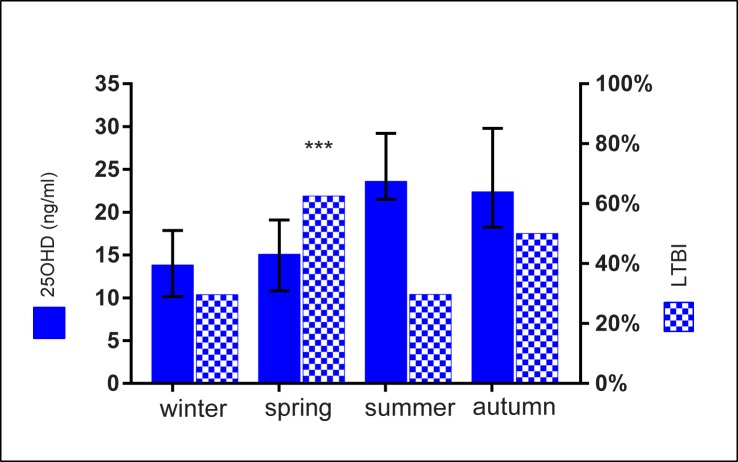
Results: Over 77% of TB cases and 62.6% of HHC had VD deficiency (<20 ng/ml). Median 25OHD concentration was significantly lower in TB cases than in HHC (11.7 vs. 18.2 ng/ml, p<0.0001). Migrants HHC had lower 25OHD levels than non-migrants (14.6 vs. 19.0 ng/ml, p = 0.026), and a trend towards a higher burden of latent TB infection (52.9% vs. 35.2%, p = 0.066). Multivariate analysis found VD deficiency in HHC was strongly associated with being sampled in winter/spring (adOR 25.68, 95%CI 7.35-89.7), corresponding to the seasons with lowest solar radiation exposure. Spring enrollment-compared with other seasons-was the chief risk factor for latent TB infection in HHC (adOR 3.14, 95%CI 1.28-7.69).
Conclusions: Hypovitaminosis D was highly prevalent in TB cases and also in HHC. A marked seasonality was found for both VD levels and latent TB in HHC, with winter being the season with lowest VD levels and spring the season with the highest risk of latent TB infection.
Conflict of interest statement
Figures
References
-
- World Health Organization (WHO). WHO | Global tuberculosis report 2016 [Internet]. WHO; 2016.
-
- Lonnroth K, Migliori GB, Abubakar I, D’Ambrosio L, de Vries G, Diel R, et al. Towards tuberculosis elimination: an action framework for low-incidence countries. Eur Respir J. 2015;45: 928–952. doi: 10.1183/09031936.00214014 - DOI - PMC - PubMed
-
- Getahun H, Matteelli A, Chaisson RE, Raviglione M. Latent Mycobacterium tuberculosis Infection. N Engl J Med. 2015;372: 2127–2135. doi: 10.1056/NEJMra1405427 - DOI - PubMed
-
- Cegielski JP, Arab L, Cornoni-Huntley J. Nutritional risk factors for tuberculosis among adults in the United States, 1971–1992. Am J Epidemiol. 2012;176: 409–22. doi: 10.1093/aje/kws007 - DOI - PMC - PubMed
-
- Bhargava A, Benedetti A, Oxlade O, Pai M, Menzies D. Undernutrition and the incidence of tuberculosis in India: national and subnational estimates of the population-attributable fraction related to undernutrition. Natl Med J India. 27: 128–33. Available: http://www.ncbi.nlm.nih.gov/pubmed/25668081 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
