

New Persistent Opioid Use After Minor and Major Surgical Procedures in US Adults
- PMID: 28403427
- PMCID: PMC7050825
- DOI: 10.1001/jamasurg.2017.0504
New Persistent Opioid Use After Minor and Major Surgical Procedures in US Adults
Erratum in
-
Errors in Analysis of New Persistent Opioid Use After Surgery.JAMA Surg. 2019 Mar 1;154(3):272. doi: 10.1001/jamasurg.2018.5476. JAMA Surg. 2019. PMID: 30624558 Free PMC article. No abstract available.
Abstract
Importance: Despite increased focus on reducing opioid prescribing for long-term pain, little is known regarding the incidence and risk factors for persistent opioid use after surgery.
Objective: To determine the incidence of new persistent opioid use after minor and major surgical procedures.
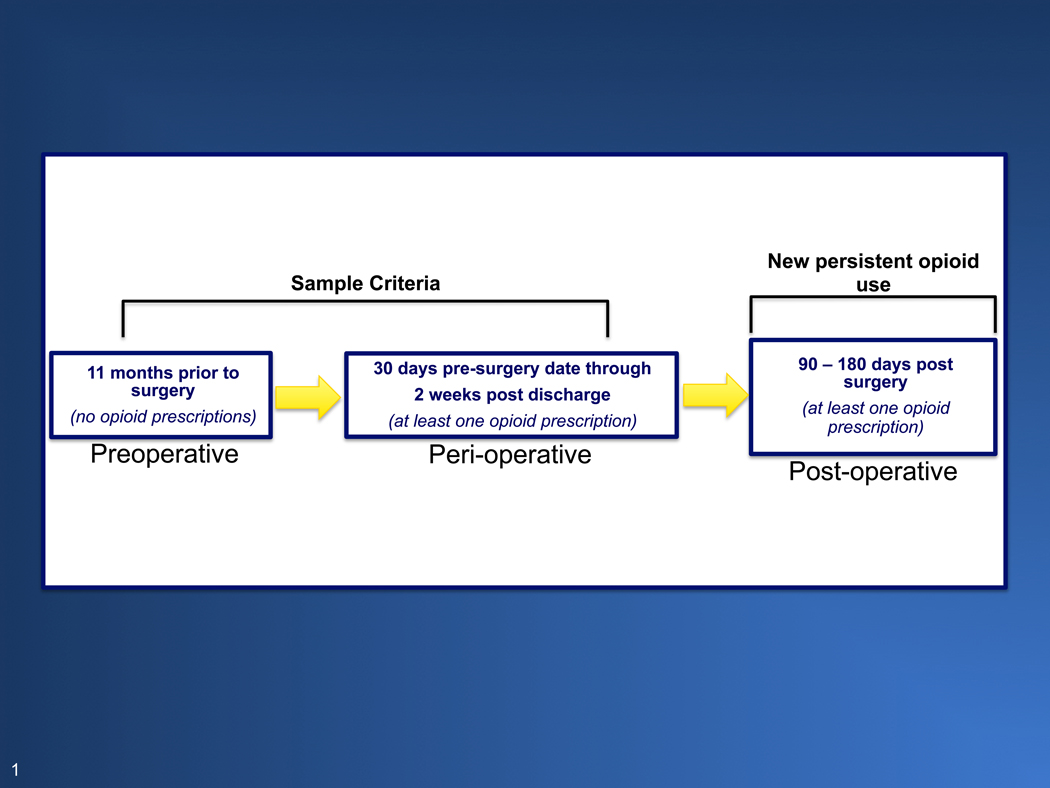
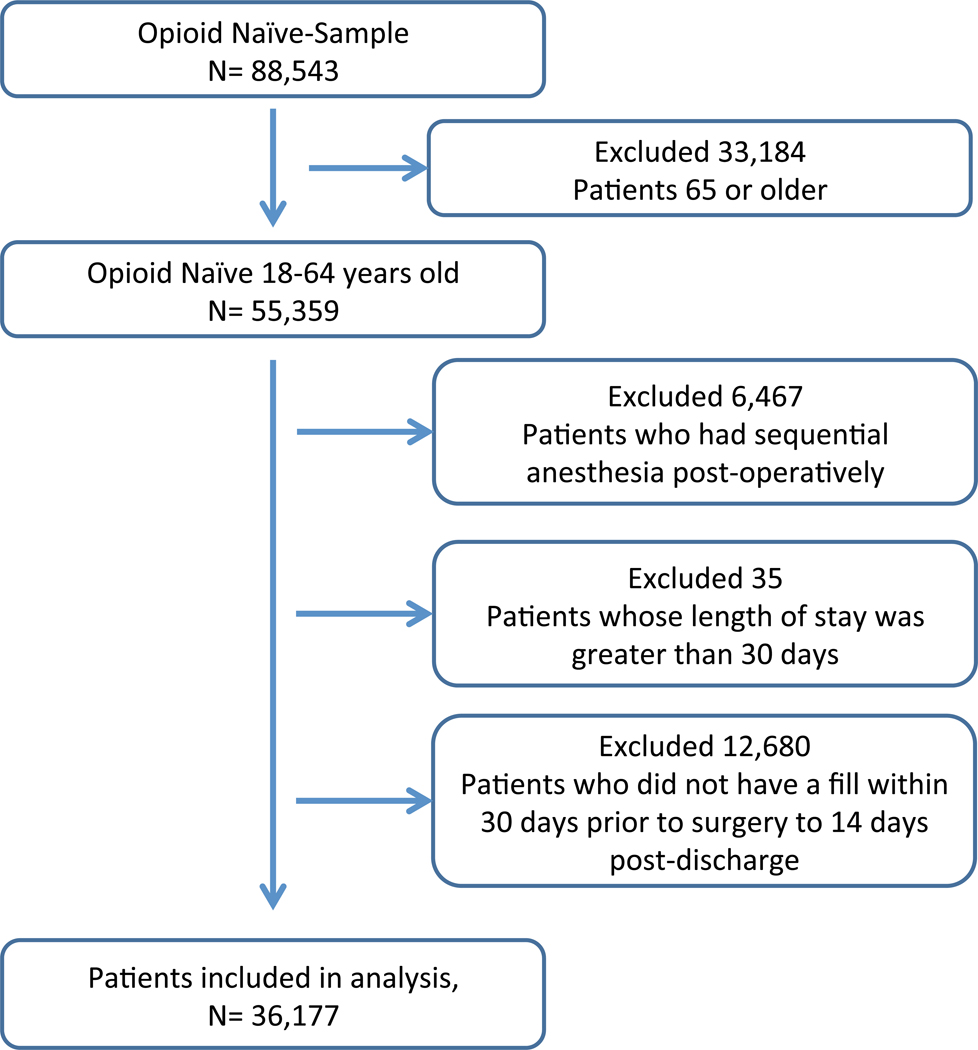
Design, setting, and participants: Using a nationwide insurance claims data set from 2013 to 2014, we identified US adults aged 18 to 64 years without opioid use in the year prior to surgery (ie, no opioid prescription fulfillments from 12 months to 1 month prior to the procedure). For patients filling a perioperative opioid prescription, we calculated the incidence of persistent opioid use for more than 90 days among opioid-naive patients after both minor surgical procedures (ie, varicose vein removal, laparoscopic cholecystectomy, laparoscopic appendectomy, hemorrhoidectomy, thyroidectomy, transurethral prostate surgery, parathyroidectomy, and carpal tunnel) and major surgical procedures (ie, ventral incisional hernia repair, colectomy, reflux surgery, bariatric surgery, and hysterectomy). We then assessed data for patient-level predictors of persistent opioid use.
Main outcomes and measures: The primary outcome was defined a priori prior to data extraction. The primary outcome was new persistent opioid use, which was defined as an opioid prescription fulfillment between 90 and 180 days after the surgical procedure.
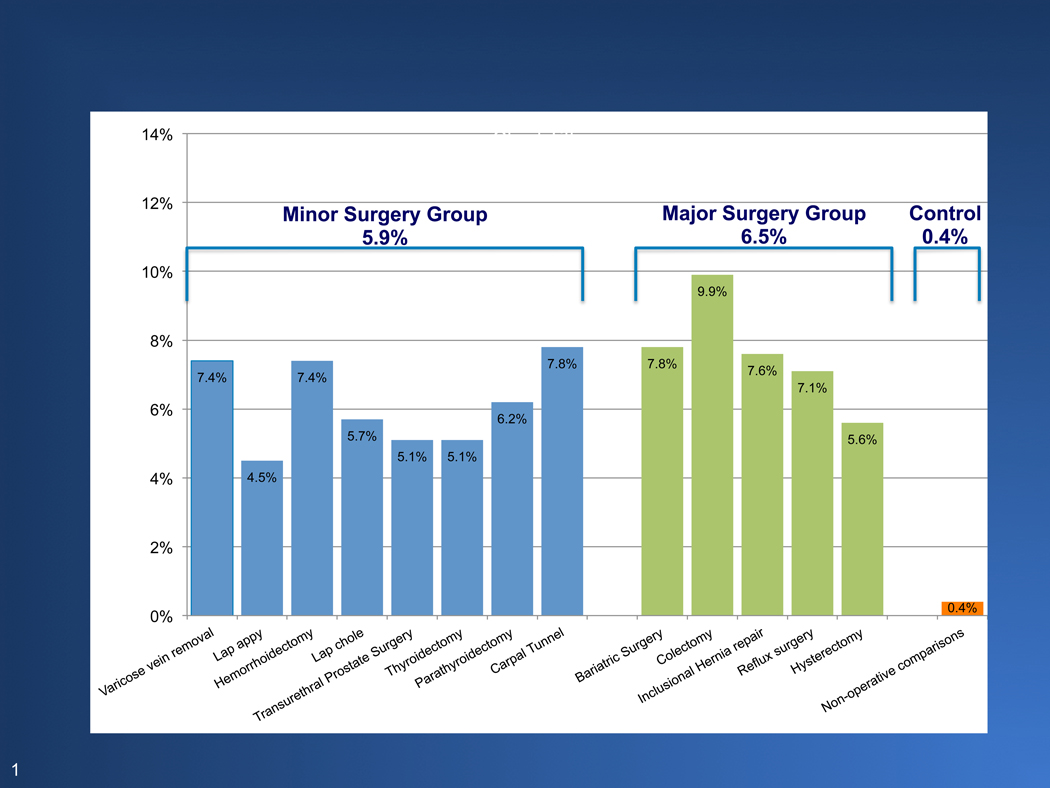
Results: A total of 36 177 patients met the inclusion criteria, with 29 068 (80.3%) receiving minor surgical procedures and 7109 (19.7%) receiving major procedures. The cohort had a mean (SD) age of 44.6 (11.9) years and was predominately female (23 913 [66.1%]) and white (26 091 [72.1%]). The rates of new persistent opioid use were similar between the 2 groups, ranging from 5.9% to 6.5%. By comparison, the incidence in the nonoperative control cohort was only 0.4%. Risk factors independently associated with new persistent opioid use included preoperative tobacco use (adjusted odds ratio [aOR], 1.35; 95% CI, 1.21-1.49), alcohol and substance abuse disorders (aOR, 1.34; 95% CI, 1.05-1.72), mood disorders (aOR, 1.15; 95% CI, 1.01-1.30), anxiety (aOR, 1.25; 95% CI, 1.10-1.42), and preoperative pain disorders (back pain: aOR, 1.57; 95% CI, 1.42-1.75; neck pain: aOR, 1.22; 95% CI, 1.07-1.39; arthritis: aOR, 1.56; 95% CI, 1.40-1.73; and centralized pain: aOR, 1.39; 95% CI, 1.26-1.54).
Conclusions and relevance: New persistent opioid use after surgery is common and is not significantly different between minor and major surgical procedures but rather associated with behavioral and pain disorders. This suggests its use is not due to surgical pain but addressable patient-level predictors. New persistent opioid use represents a common but previously underappreciated surgical complication that warrants increased awareness.
Figures
Comment in
-
Errors in Analysis in Study of New Persistent Opioid Use After Surgery.JAMA Surg. 2019 Mar 1;154(3):268-269. doi: 10.1001/jamasurg.2018.5299. JAMA Surg. 2019. PMID: 30624569 No abstract available.
References
-
- Cullen KA, Hall MJ, Golosinskiy A. Ambulatory surgery in the United States, 2006. Natl Health Stat Report. 2009(11):1–25. - PubMed
-
- Russo A, Elixhauser A, Steiner C, Wier L. Hospital-Based Ambulatory Surgery, 2007: Statistical Brief #86. 2006. - PubMed
-
- Birkmeyer JD. Progress and challenges in improving surgical outcomes. Br J Surg. 2012;99(11):1467–1469. - PubMed
-
- Finks JF, Kole KL, Yenumula PR, et al. Predicting risk for serious complications with bariatric surgery: results from the Michigan Bariatric Surgery Collaborative. Ann Surg. 2011;254(4):633–640. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
