

Clinical pathophysiology of hypoxic ischemic brain injury after cardiac arrest: a "two-hit" model
- PMID: 28403909
- PMCID: PMC5390465
- DOI: 10.1186/s13054-017-1670-9
Clinical pathophysiology of hypoxic ischemic brain injury after cardiac arrest: a "two-hit" model
Abstract
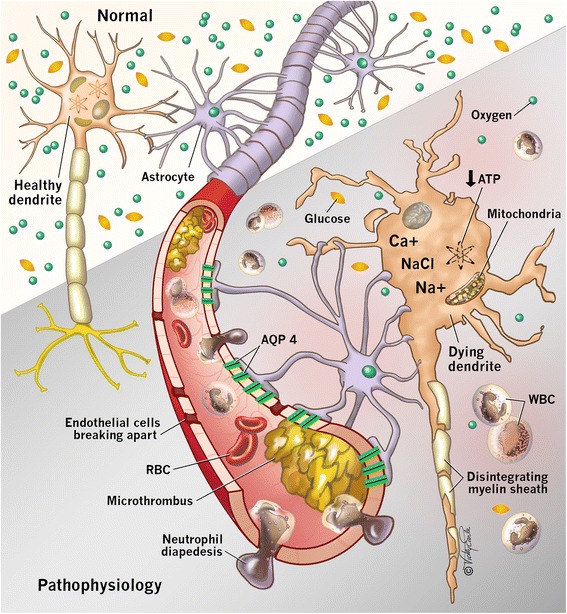
Hypoxic ischemic brain injury (HIBI) after cardiac arrest (CA) is a leading cause of mortality and long-term neurologic disability in survivors. The pathophysiology of HIBI encompasses a heterogeneous cascade that culminates in secondary brain injury and neuronal cell death. This begins with primary injury to the brain caused by the immediate cessation of cerebral blood flow following CA. Thereafter, the secondary injury of HIBI takes place in the hours and days following the initial CA and reperfusion. Among factors that may be implicated in this secondary injury include reperfusion injury, microcirculatory dysfunction, impaired cerebral autoregulation, hypoxemia, hyperoxia, hyperthermia, fluctuations in arterial carbon dioxide, and concomitant anemia.Clarifying the underlying pathophysiology of HIBI is imperative and has been the focus of considerable research to identify therapeutic targets. Most notably, targeted temperature management has been studied rigorously in preventing secondary injury after HIBI and is associated with improved outcome compared with hyperthermia. Recent advances point to important roles of anemia, carbon dioxide perturbations, hypoxemia, hyperoxia, and cerebral edema as contributing to secondary injury after HIBI and adverse outcomes. Furthermore, breakthroughs in the individualization of perfusion targets for patients with HIBI using cerebral autoregulation monitoring represent an attractive area of future work with therapeutic implications.We provide an in-depth review of the pathophysiology of HIBI to critically evaluate current approaches for the early treatment of HIBI secondary to CA. Potential therapeutic targets and future research directions are summarized.
Keywords: Anemia; Carbon dioxide; Cardiac arrest; Cerebral edema; Cerebral oxygen delivery; Hypothermia; Hypoxic ischemic brain injury; Normobaric hyperoxia; Targeted temperature management.
Figures
Comment in
-
Targeted therapeutic mild hypercapnia after cardiac arrest.Crit Care. 2017 Jul 31;21(1):196. doi: 10.1186/s13054-017-1770-6. Crit Care. 2017. PMID: 28756765 Free PMC article. No abstract available.
-
Targeted therapeutic mild hypercapnia after cardiac arrest: a part of the bundle of care for mitigating secondary injury after cardiac arrest.Crit Care. 2017 Sep 7;21(1):236. doi: 10.1186/s13054-017-1825-8. Crit Care. 2017. PMID: 28882169 Free PMC article. No abstract available.
References
-
- Gräsner JT, Lefering R, Koster RW, Masterson S, Böttiger BW, Herlitz J, et al. EuReCa ONE—27 Nations, ONE Europe, ONE Registry: a prospective one month analysis of out-of-hospital cardiac arrest outcomes in 27 countries in Europe. Resuscitation. 2016;105:188–95. doi: 10.1016/j.resuscitation.2016.06.004. - DOI - PubMed
-
- Nolan JP, Neumar RW, Adrie C, Aibiki M, Berg RA, Böttiger BW, et al. Post-cardiac arrest syndrome: epidemiology, pathophysiology, treatment, and prognostication. A Scientific Statement from the International Liaison Committee on Resuscitation; the American Heart Association Emergency Cardiovascular Care Committee; the Council on Cardiovascular Surgery and Anesthesia; the Council on Cardiopulmonary, Perioperative, and Critical Care; the Council on Stroke. Resuscitation. 2008;79:350–79. doi: 10.1016/j.resuscitation.2008.09.017. - DOI - PubMed
-
- Bunch TJ, White RD, Smith GE, Hodge DO, Gersh BJ, Hammill SC, et al. Long-term subjective memory function in ventricular fibrillation out-of-hospital cardiac arrest survivors resuscitated by early defibrillation. Resuscitation. 2004;60:189–95. doi: 10.1016/j.resuscitation.2003.09.010. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
