

Immediate Mood Scaler: Tracking Symptoms of Depression and Anxiety Using a Novel Mobile Mood Scale
- PMID: 28404542
- PMCID: PMC5406620
- DOI: 10.2196/mhealth.6544
Immediate Mood Scaler: Tracking Symptoms of Depression and Anxiety Using a Novel Mobile Mood Scale
Abstract
Background: Mood disorders are dynamic disorders characterized by multimodal symptoms. Clinical assessment of symptoms is currently limited to relatively sparse, routine clinic visits, requiring retrospective recollection of symptoms present in the weeks preceding the visit. Novel advances in mobile tools now support ecological momentary assessment of mood, conducted frequently using mobile devices, outside the clinical setting. Such mood assessment may help circumvent problems associated with infrequent reporting and better characterize the dynamic presentation of mood symptoms, informing the delivery of novel treatment options.
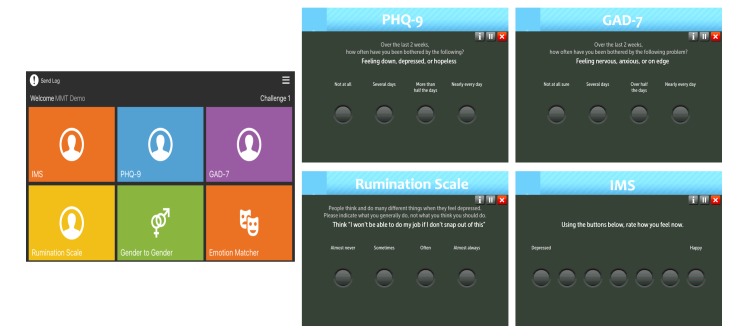
Objectives: The aim of our study was to validate the Immediate Mood Scaler (IMS), a newly developed, iPad-deliverable 22-item self-report tool designed to capture current mood states.
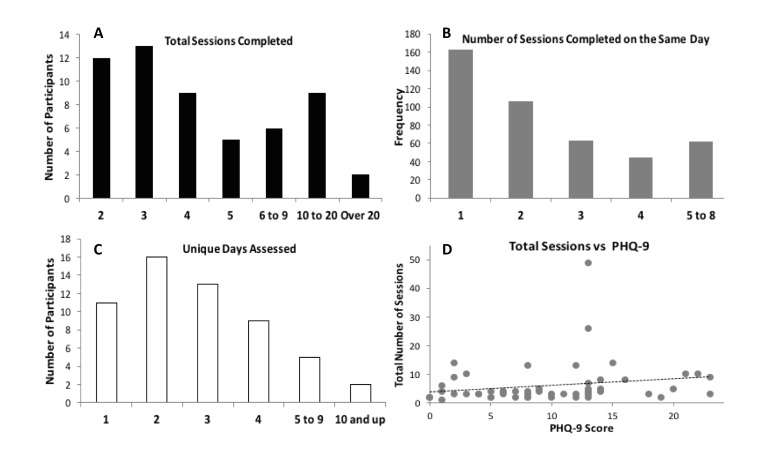
Methods: A total of 110 individuals completed standardized questionnaires (Patient Health Questionnaire, 9-item [PHQ-9]; generalized anxiety disorder, 7-Item [GAD-7]; and rumination scale) and IMS at baseline. Of the total, 56 completed at least one additional session of IMS, and 17 completed one additional administration of PHQ-9 and GAD-7. We conducted exploratory Principal Axis Factor Analysis to assess dimensionality of IMS, and computed zero-order correlations to investigate associations between IMS and standardized scales. Linear Mixed Model (LMM) was used to assess IMS stability across time and to test predictability of PHQ-9 and GAD-7 score by IMS.
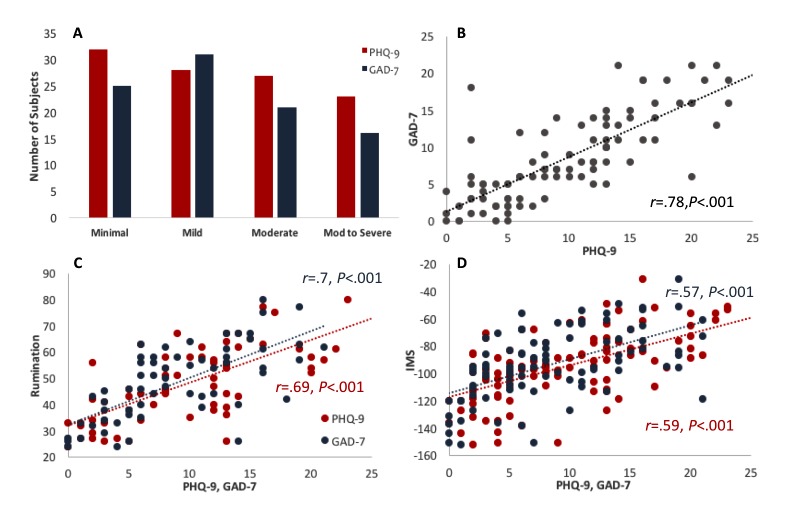
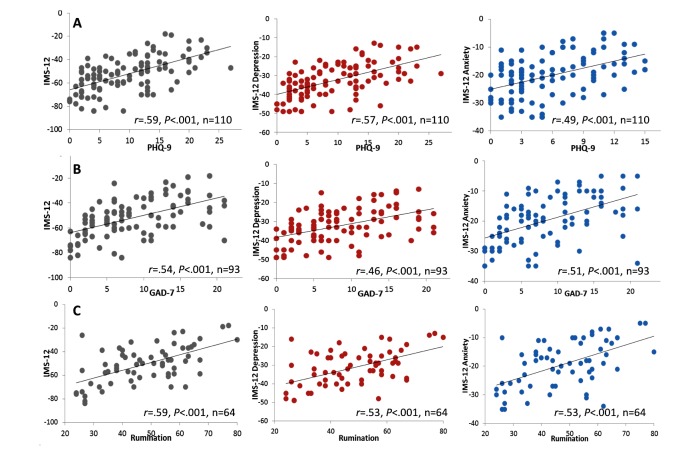
Results: Strong correlations were found between standard mood scales and the IMS at baseline (r=.57-.59, P<.001). A factor analysis revealed a 12-item IMS ("IMS-12") with two factors: a "depression" factor and an "anxiety" factor. IMS-12 depression subscale was more strongly correlated with PHQ-9 than with GAD-7 (z=1.88, P=.03), but the reverse pattern was not found for IMS-12 anxiety subscale. IMS-12 showed less stability over time compared with PHQ-9 and GAD-7 (.65 vs .91), potentially reflecting more sensitivity to mood dynamics. In addition, IMS-12 ratings indicated that individuals with mild to moderate depression had greater mood fluctuations compared with individuals with severe depression (.42 vs .79; P=.04). Finally, IMS-12 significantly contributed to the prediction of subsequent PHQ-9 (beta=1.03, P=.02) and GAD-7 scores (beta =.93, P=.01).
Conclusions: Collectively, these data suggest that the 12-item IMS (IMS-12) is a valid tool to assess momentary mood symptoms related to anxiety and depression. Although IMS-12 shows good correlation with standardized scales, it further captures mood fluctuations better and significantly adds to the prediction of the scales. Results are discussed in the context of providing continuous symptom quantification that may inform novel treatment options and support personalized treatment plans.
Keywords: anxiety; depression; ecological momentary assessment; mobile; mood disorders.
©Mor Nahum, Thomas M Van Vleet, Vikaas S Sohal, Julie J Mirzabekov, Vikram R Rao, Deanna L Wallace, Morgan B Lee, Heather Dawes, Alit Stark-Inbar, Joshua Thomas Jordan, Bruno Biagianti, Michael Merzenich, Edward F Chang. Originally published in JMIR Mhealth and Uhealth (http://mhealth.jmir.org), 12.04.2017.
Conflict of interest statement
Conflicts of Interest: Authors Tom Van Vleet, Bruno Biagianti, and Michael Merzenich are all paid employees of Posit Science, a commercial company which develops the mobile mood tracking app and the IMS in particular. Author Mor Nahum is a paid consultant of Posit Science. None of the other authors have any financial interest in Posit Science.
Figures
References
-
- Ferrari AJ, Charlson FJ, Norman RE, Patten SB, Freedman G, Murray CJ, Vos T, Whiteford HA. Burden of depressive disorders by country, sex, age, and year: findings from the global burden of disease study 2010. PLoS Med. 2013 Nov;10(11):e1001547. doi: 10.1371/journal.pmed.1001547. http://dx.plos.org/10.1371/journal.pmed.1001547 PMEDICINE-D-13-01260 - DOI - DOI - PMC - PubMed
-
- Greenberg PE, Kessler RC, Birnbaum HG, Leong SA, Lowe SW, Berglund PA, Corey-Lisle PK. The economic burden of depression in the United States: how did it change between 1990 and 2000? J Clin Psychiatry. 2003 Dec;64(12):1465–75. - PubMed
-
- Torres ER. Disability and comorbidity among major depressive disorder and double depression in African-American adults. J Affect Disord. 2013 Sep 25;150(3):1230–3. doi: 10.1016/j.jad.2013.05.089. http://europepmc.org/abstract/MED/23809403 S0165-0327(13)00468-0 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
