

Combined antiangiogenic and anti-PD-L1 therapy stimulates tumor immunity through HEV formation
- PMID: 28404866
- PMCID: PMC5554432
- DOI: 10.1126/scitranslmed.aak9679
Combined antiangiogenic and anti-PD-L1 therapy stimulates tumor immunity through HEV formation
Abstract
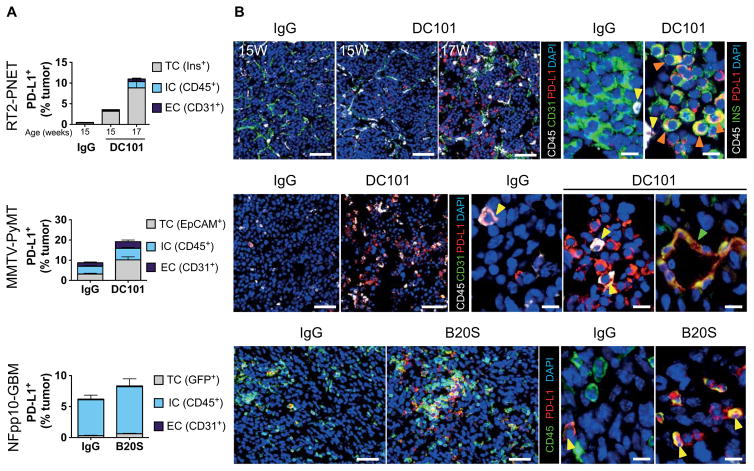
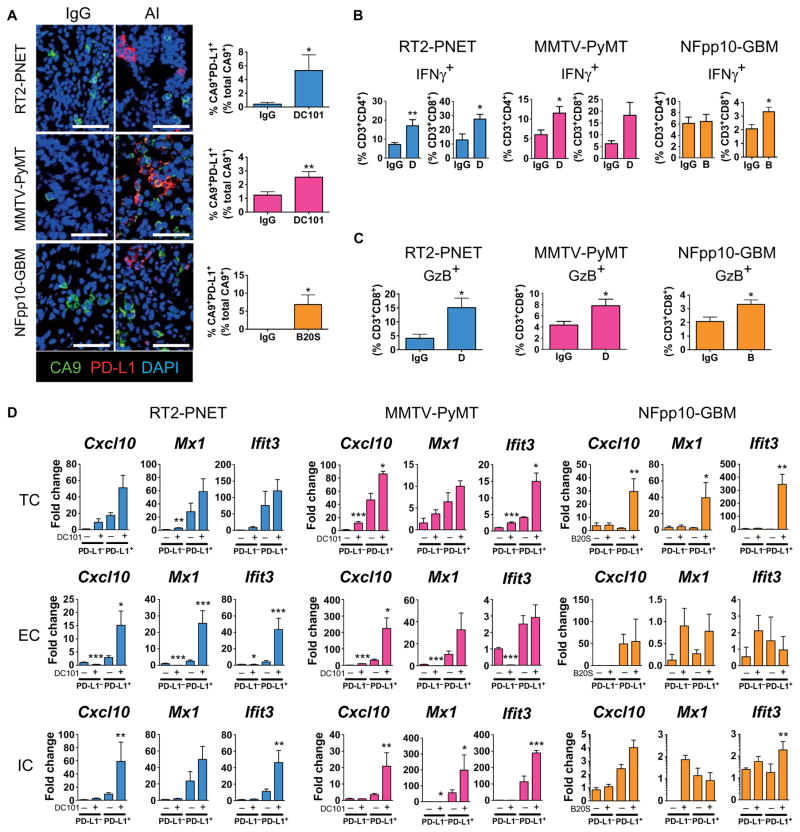
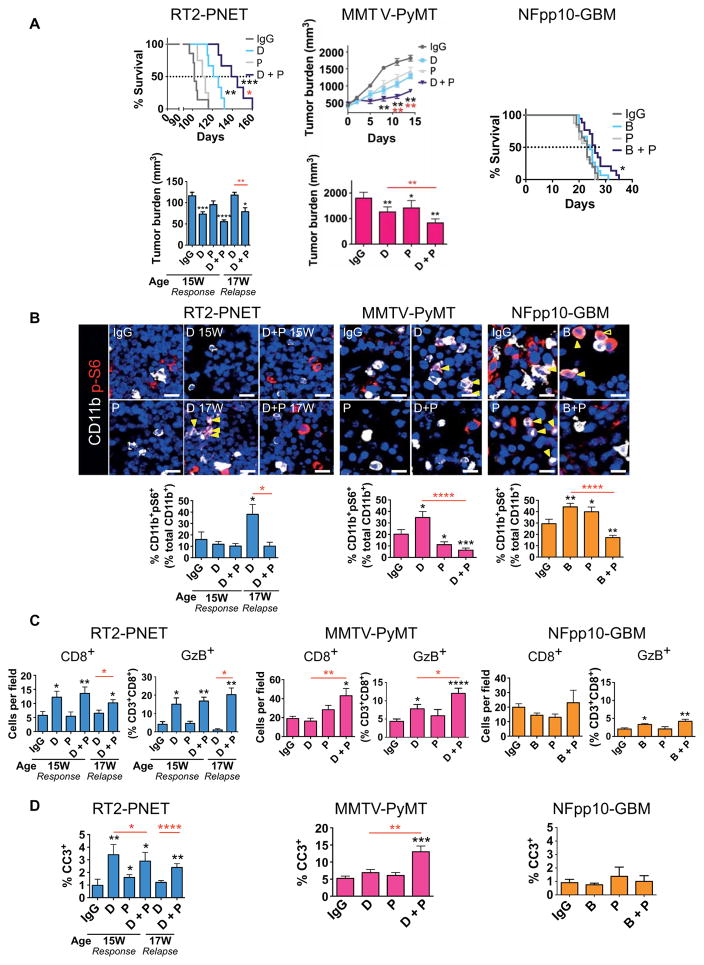
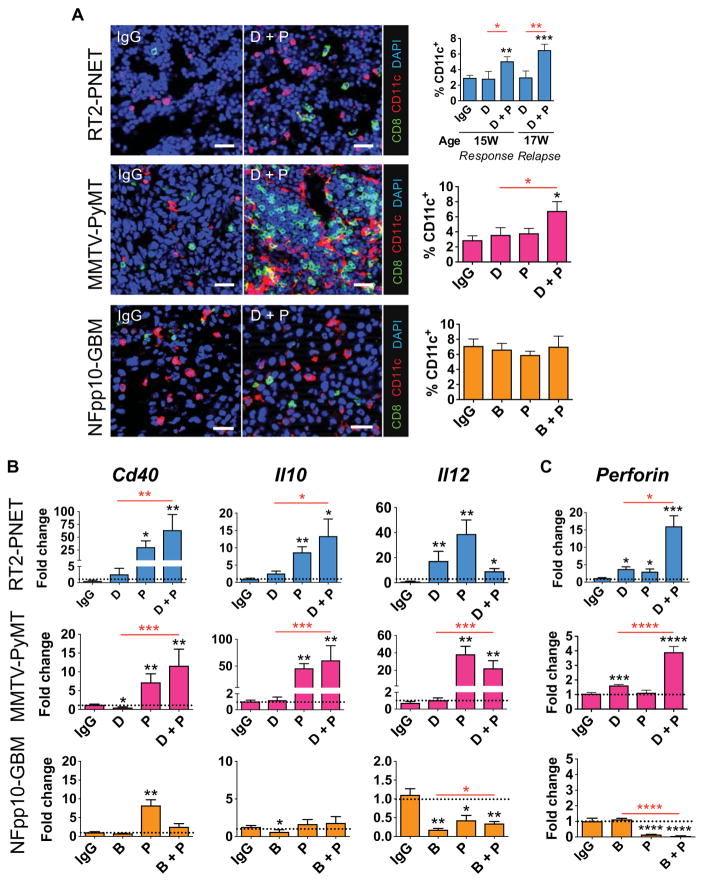
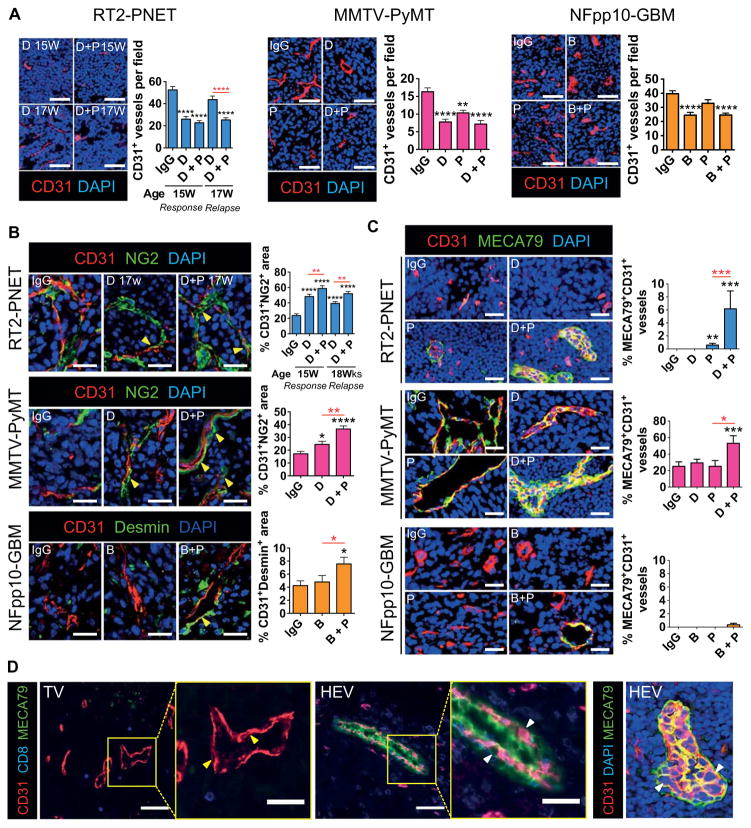
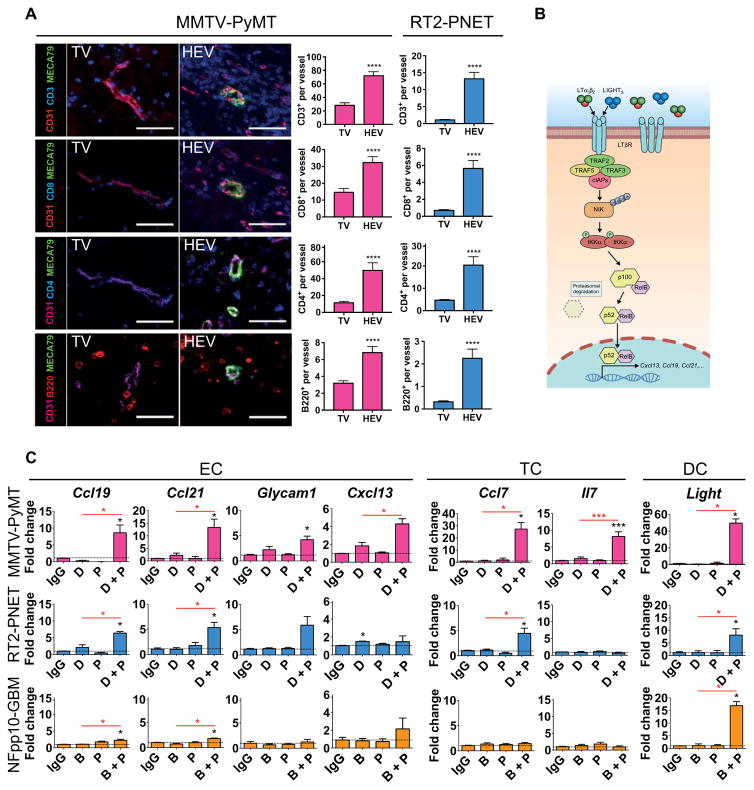
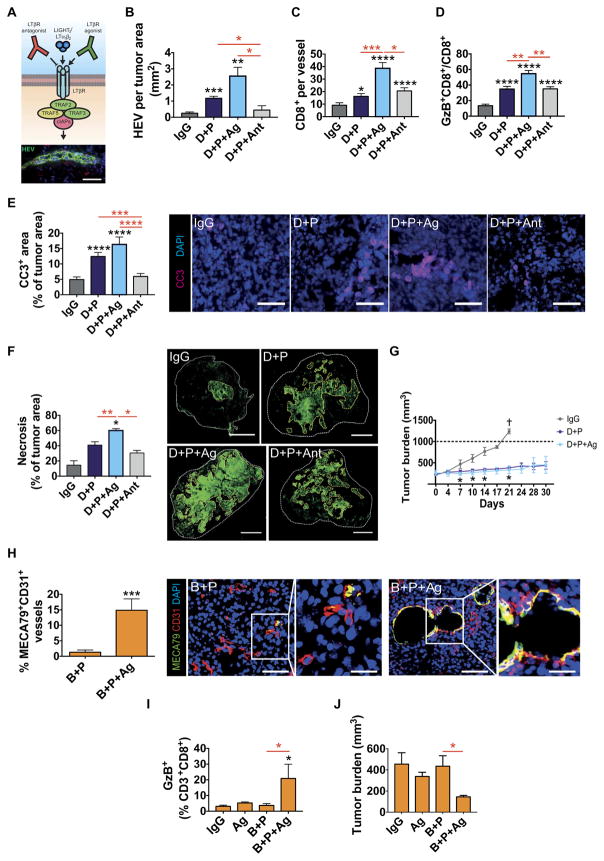
Inhibitors of VEGF (vascular endothelial growth factor)/VEGFR2 (vascular endothelial growth factor receptor 2) are commonly used in the clinic, but their beneficial effects are only observed in a subset of patients and limited by induction of diverse relapse mechanisms. We describe the up-regulation of an adaptive immunosuppressive pathway during antiangiogenic therapy, by which PD-L1 (programmed cell death ligand 1), the ligand of the negative immune checkpoint regulator PD-1 (programmed cell death protein 1), is enhanced by interferon-γ-expressing T cells in distinct intratumoral cell types in refractory pancreatic, breast, and brain tumor mouse models. Successful treatment with a combination of anti-VEGFR2 and anti-PD-L1 antibodies induced high endothelial venules (HEVs) in PyMT (polyoma middle T oncoprotein) breast cancer and RT2-PNET (Rip1-Tag2 pancreatic neuroendocrine tumors), but not in glioblastoma (GBM). These HEVs promoted lymphocyte infiltration and activity through activation of lymphotoxin β receptor (LTβR) signaling. Further activation of LTβR signaling in tumor vessels using an agonistic antibody enhanced HEV formation, immunity, and subsequent apoptosis and necrosis in pancreatic and mammary tumors. Finally, LTβR agonists induced HEVs in recalcitrant GBM, enhanced cytotoxic T cell (CTL) activity, and thereby sensitized tumors to antiangiogenic/anti-PD-L1 therapy. Together, our preclinical studies provide evidence that anti-PD-L1 therapy can sensitize tumors to antiangiogenic therapy and prolong its efficacy, and conversely, antiangiogenic therapy can improve anti-PD-L1 treatment specifically when it generates intratumoral HEVs that facilitate enhanced CTL infiltration, activity, and tumor cell destruction.
Copyright © 2017, American Association for the Advancement of Science.
Conflict of interest statement
Figures
Comment in
-
Cancer immunotherapy: T cells get a ride.Nat Rev Drug Discov. 2017 Jun;16(6):383. doi: 10.1038/nrd.2017.103. Epub 2017 May 19. Nat Rev Drug Discov. 2017. PMID: 28529320 No abstract available.
-
Immunotherapy: T cells get a ride.Nat Rev Cancer. 2017 May 24;17(6):333. doi: 10.1038/nrc.2017.39. Nat Rev Cancer. 2017. PMID: 28536454 No abstract available.
-
Antiangiogenic therapy and immune checkpoint blockade go hand in hand.Ann Transl Med. 2017 Dec;5(24):497. doi: 10.21037/atm.2017.10.12. Ann Transl Med. 2017. PMID: 29299458 Free PMC article. No abstract available.
References
-
- Hanahan D, Weinberg RA. Hallmarks of cancer: The next generation. Cell. 2011;144:646–674. - PubMed
-
- Motz GT, Coukos G. The parallel lives of angiogenesis and immunosuppression: Cancer and other tales. Nat Rev Immunol. 2011;11:702–711. - PubMed
-
- Mahoney KM, Rennert PD, Freeman GJ. Combination cancer immunotherapy and new immunomodulatory targets. Nat Rev Drug Discov. 2015;14:561–584. - PubMed
-
- Callahan MK, Postow MA, Wolchok JD. Targeting T cell co-receptors for cancer therapy. Immunity. 2016;44:1069–1078. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
