Rapidity and efficacy of ultrasonographic sliding lung sign and auscultation in confirming endotracheal intubation in overweight and obese patients
- PMID: 28405036
- PMCID: PMC5372403
- DOI: 10.4103/0019-5049.202164
Rapidity and efficacy of ultrasonographic sliding lung sign and auscultation in confirming endotracheal intubation in overweight and obese patients
Abstract
Background and aims: Obese individuals are predisposed to difficult airway and intubation. They usually yield confusing or misleading auscultatory findings. We aimed to assess the rapidity and efficacy of ultrasonographic (USG) sliding lung sign for confirming endotracheal intubation in normal as well as overweight and obese surgical patients.
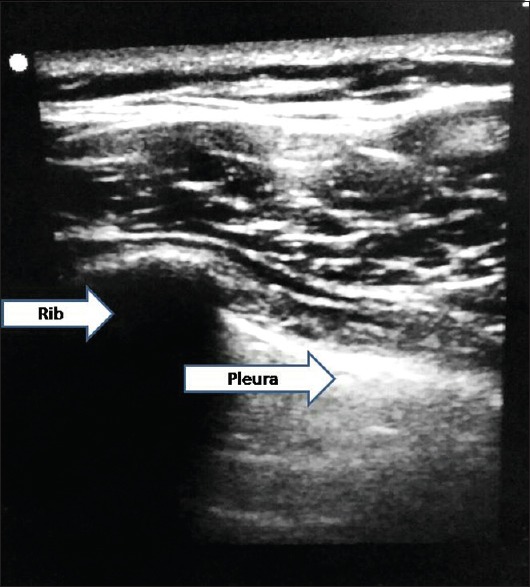
Methods: This prospective, observational study was performed in forty surgical patients. Twenty patients with body mass index (BMI) <25 were recruited to Group A, whereas twenty patients with BMI ≥25 constituted Group B. Following induction and intubation, appearance of end-tidal carbon dioxide waveform was used to confirm endotracheal intubation. Presence of breath sounds bilaterally was sought by auscultation, and time taken for auscultatory confirmation was noted. The USG confirmation of air entry to the lung field as indicated by lung sliding was sought, and the time taken was noted. Chi-square test, independent t-test and paired t-test were used as applicable.
Results: Auscultatory confirmation was more rapid in Group A as compared to Group B (9.34 ± 2.43 s vs. 14.35 ± 5.53 s, P = 0.001). However, there was no significant difference in USG confirmation time in both the groups (8.57 ± 2.05 s vs. 8.61 ± 1.66 s). Four patients in Group B had doubtful breath sounds against none in Group A. There was no doubtful lung slide with USG in both groups. One case of endobronchial intubation in Group B was diagnosed with USG which was doubtful by auscultation.
Conclusion: Ultrasound directed confirmation of endotracheal tube placement in overweight and obese patients is superior in speed and accuracy in comparison to the standard auscultatory method.
Keywords: Auscultation; endotracheal intubation; obesity; sliding lung sign; ultrasonography.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Juvin P, Lavaut E, Dupont H, Lefevre P, Demetriou M, Dumoulin JL, et al. Difficult tracheal intubation is more common in obese than in lean patients. Anesth Analg. 2003;97:595–600. - PubMed
-
- Adams JP, Murphy PG. Obesity in anaesthesia and intensive care. Br J Anaesth. 2000;85:91–108. - PubMed
-
- Weaver B, Lyon M, Blaivas M. Confirmation of endotracheal tube placement after intubation using the ultrasound sliding lung sign. Acad Emerg Med. 2006;13:239–44. - PubMed
-
- Sim SS, Lien WC, Chou HC, Chong KM, Liu SH, Wang CH, et al. Ultrasonographic lung sliding sign in confirming proper endotracheal intubation during emergency intubation. Resuscitation. 2012;83:307–12. - PubMed
-
- Álvarez-Díaz N, Amador-García I, Fuentes-Hernández M, Dorta-Guerra R. Comparison between transthoracic lung ultrasound and a clinical method in confirming the position of double-lumen tube in thoracic anaesthesia. A pilot study. Rev Esp Anestesiol Reanim. 2015;62:305–12. - PubMed