

Diagnosis of sarcoidosis from a biopsy of a dilated mammary duct
- PMID: 28405081
- PMCID: PMC5349827
- DOI: 10.1080/08998280.2017.11929584
Diagnosis of sarcoidosis from a biopsy of a dilated mammary duct
Abstract
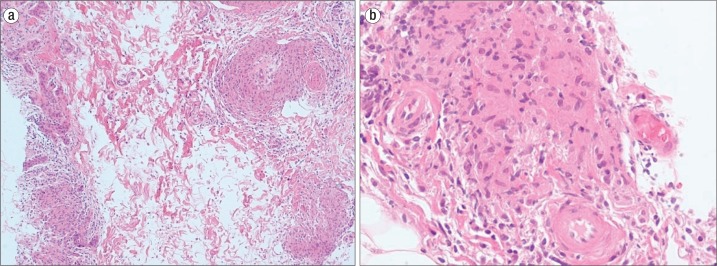
Sarcoidosis is an immunologic disease of unknown etiology that manifests most frequently within the lungs or associated lymph nodes. Sarcoidosis involving the breast is seen in <1% of cases and usually is diagnosed in patients with multisystem disease. The clinical and imaging presentations of sarcoidosis of the breast can be variable. Though uncommon, sarcoidosis should be considered in the differential diagnosis of a breast lesion, and given that imaging characteristics cannot distinguish between sarcoidosis and malignancy, all breast lesions in patients with sarcoidosis should be biopsied. Our case study demonstrates a diagnosis of sarcoidosis in an asymptomatic patient presenting with a single dilated duct and associated filling defect within the right breast.
Figures


References
-
- Baughman RP, Teirstein AS, Judson MA, Rossman MD, Yeager H Jr, Bresnitz EA, DePalo L, Hunninghake G, Iannuzzi MC, Johns CJ, McLennan G, Moller DR, Newman LS, Rabin DL, Rose C, Rybicki B, Weinberger SE, Terrin ML, Knatterud GL, Cherniak R. Clinical characteristics of patients in a case control study of sarcoidosis. Am J Respir Crit Care Med. 2001;164(10 Pt 1):1885–1889. - PubMed
-
- Donaldson BA, Polynice A, Oluwole S. Sarcoidosis of the breast: case report and chart review. Am Surg. 1995;61(9):778–780. - PubMed
-
- Ojeda H, Sardi A, Totoonchie A. Sarcoidosis of the breast: implications for the general surgeon. Am Surg. 2000;66(12):1144–1148. - PubMed
-
- Sabaté JM, Clotet M, Gómez A, De Las Heras P, Torrubia S, Salinas T. Radiologic evaluation of uncommon inflammatory and reactive breast disorders. Radiographics. 2005;25(2):411–424. - PubMed
-
- Kenzel PP, Hadijuana J, Hosten N, Minguillon C, Oellinger H, Siewert C, Thiel T, Lichtenegger W, Felix R. Boeck sarcoidosis of the breast: mammographic ultrasound, and MR findings. J Comput Assist Tomogr. 1997;21(3):439–441. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources