

The use of enteral access for continuous delivery of levodopa-carbidopa in patients with advanced Parkinson's disease
- PMID: 28405323
- PMCID: PMC5384558
- DOI: 10.1177/2050640616650804
The use of enteral access for continuous delivery of levodopa-carbidopa in patients with advanced Parkinson's disease
Abstract
Background: Continuous delivery to the jejunum of levodopa-carbidopa is a promising therapy in patients with advanced Parkinson's disease, as it reduces motor fluctuation. Percutaneous endoscopic gastrostomy and jejunal tube (PEG-J) placement is a suitable option for this. However, studies focused in PEG-J management are lacking.
Objectives: We report our experience regarding this technique, including technical success, adverse events and outcomes, in patients with advanced Parkinson's disease.
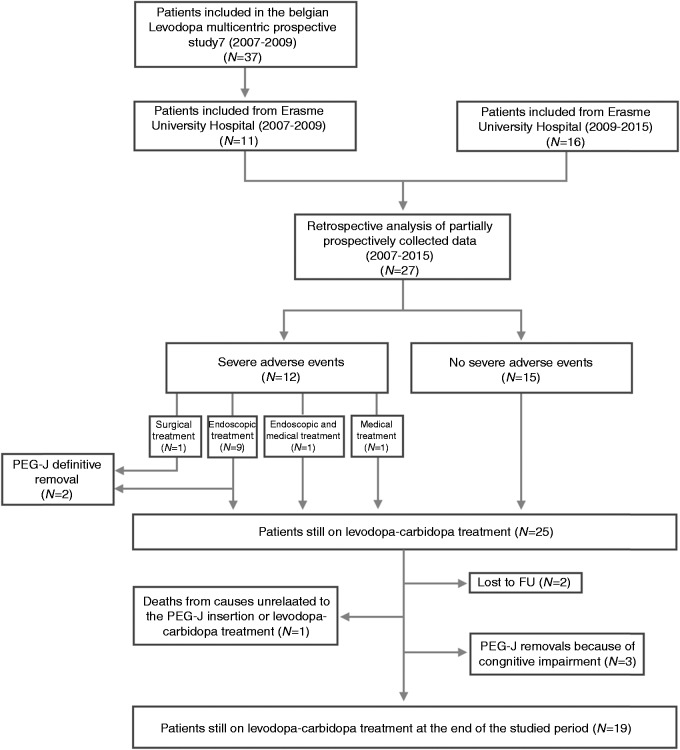
Methods: Twenty-seven advanced Parkinson's disease patients (17 men, median age: 64 years, median disease duration: 11 years) were included in a retrospective study from June 2007 to April 2015. The median follow-up period was 48 months (1-96).
Results: No adverse events were noted during and after nasojejunal tube insertion (to assess treatment efficacy). After a good therapeutic response, a PEG-J was placed successfully in all patients. The PEG tube was inserted according to Ponsky's method. The jejunal extension was inserted during the same procedure in all patients. Twelve patients (44%) experienced severe adverse events related to the PEG-J insertion, which occurred after a median follow-up of 15.5 months. Endoscopy was the main treatment modality. Patients who experienced severe adverse events had a higher comorbidity score (p = 0.011) but were not older (p = 0.941) than patients who did not.
Conclusions: While all patients responded well to levodopa-carbidopa regarding neurological outcomes, gastro-intestinal severe adverse events were frequent and related to comorbidities. Endoscopic treatment is the cornerstone for management of PEG-J related events. In conclusion, clinicians and endoscopists, as well as patients, should be fully informed of procedure-related adverse events and patients should be followed in centres experienced in their management.
Keywords: PEG; PEG-J; Parkinson’s disease; adverse events; duodopa; levodopa; percutaneous endoscopic gastrostomy and jejunal tube.
Figures
References
-
- Hardoff R, Sula M, Tamir A, et al. Gastric emptying time and gastric motility in patients with Parkinson’s disease. Mov Disord 2001; 16: 1041–1047. - PubMed
-
- Nyholm D. Duodopa® treatment for advanced Parkinson’s disease: A review of efficacy and safety. Parkinsonism Relat Disord 2012; 18: 916–929. - PubMed
-
- Clarke CE, Worth P, Grosset D, et al. Systematic review of apomorphine infusion, levodopa infusion and deep brain stimulation in advanced Parkinson’s disease. Parkinsonism Relat Disord 2009; 15: 728–741. - PubMed
-
- Negreanu L, Popescu BO, Babiuc RD, et al. Duodopa infusion treatment: A point of view from the gastroenterologist. J Gastrointestin Liver Disord 2011; 20: 325–327. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
