

Histopathological correlations to ureteral lesions visualized during ureteroscopy
- PMID: 28405762
- PMCID: PMC5613101
- DOI: 10.1007/s00345-017-2035-3
Histopathological correlations to ureteral lesions visualized during ureteroscopy
Abstract
Purpose: To correlate ureteral lesions visualized during ureteroscopy with histopathological findings.
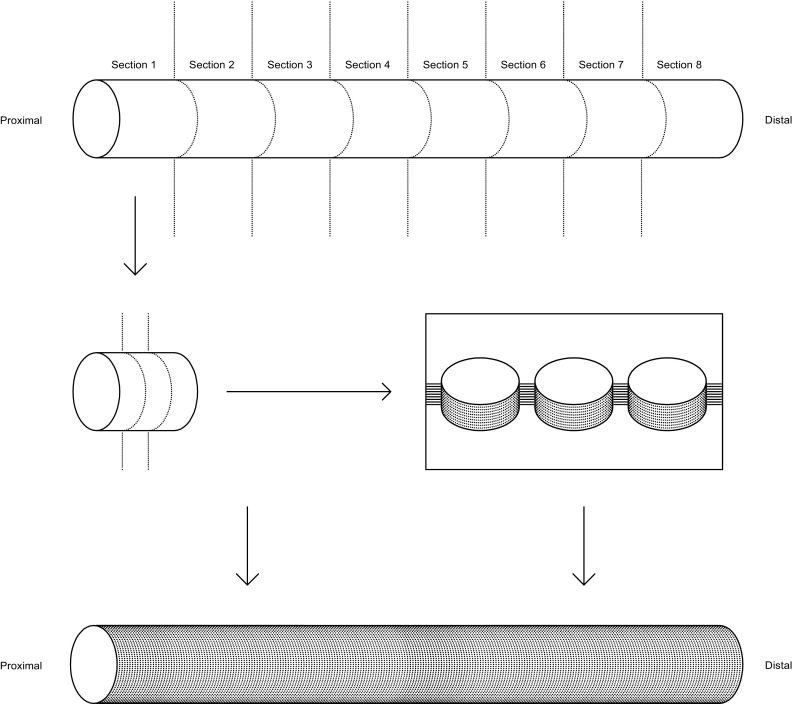
Materials and methods: Ureteral access sheaths (UAS) sized 13/15 Fr. were inserted bilaterally in 22 laboratory pigs. During retraction of the UAS with a semirigid ureteroscope inside, ureteral lesions were evaluated and registered using the Post-ureteroscopic lesion scale (PULS). Ureters were excised in vivo between the uretero-pelvic junction and the uretero-vesical junction. Embedded in paraffin, 4-µm thick sections were step sectioned at 250-300 µm intervals and haematoxylin and eosin (HE) stained. Histopathological scoring of ureteral wall lesions was subsequently performed according to PULS.
Results: In 72.1% of ureters, the highest histopathological score was at least 1 grade higher than the highest endoscopic PULS score. For 12 (27.9%) lesions, the difference was 2 scores higher, and for 1 (2.3%), it was 3 scores higher. The histopathological PULS grade was higher than the endoscopical PULS grade at all minimum, quartile, and maximum scores. There was a significant difference in the distribution of highest lesional scores between the endoscopic and histopathological PULS (p = 0.002). The calculated mean of the highest scores was 1.49 for endoscopic PULS and 2.51 for histopathological PULS (p < 0.0001).
Conclusion: Histopathological evaluation of ureteral wall lesions after UAS placement revealed a significantly higher degree of severity than observed endoscopically. Thus, endoscopy underestimated the histopathological extent of the lesion in the majority of cases.
Keywords: Complications; Histopathology; Post-ureteroscopic lesion scale; Ureteral access sheath; Ureteral lesions; Ureteroscopy.
Conflict of interest statement
Funding
The Japanese-Swedish Research Foundation and the Research Foundation of Lillebaelt Hospital supported the study, but had no influence on study design, performance, analysis of data and publication.
Conflict of interest
K.H. Andreassen has received speaker honoraria from Boston Scientific. P.J.S. Osther is member of advisory boards of Olympus, Boston Scientific, and Coloplast. P.J.S. Osther has received speaker honoraria from Olympus, Cook Medical, Boston Scientific, Karl Storz Endoskope, and Coloplast.
Human and animal rights statement
The research did not involve human participants. The animal studies complied with national ethical standards, and the protocols were approved by The National Animal Experiments Inspectorate (Copenhagen, Denmark) (Animal approved project number 2014-15-2934-01015).
Informed consent
N.A. (the study did not involve human participants).
Figures


References
-
- Traxer O, Thomas A. Prospective evaluation and classification of ureteral wall injuries resulting from insertion of a ureteral access sheath during retrograde intrarenal surgery. J Urol Elsevier Inc. 2013;189(2):580–584. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
