

Anthracyclines induce early changes in left ventricular systolic and diastolic function: A single centre study
- PMID: 28407011
- PMCID: PMC5391073
- DOI: 10.1371/journal.pone.0175544
Anthracyclines induce early changes in left ventricular systolic and diastolic function: A single centre study
Abstract
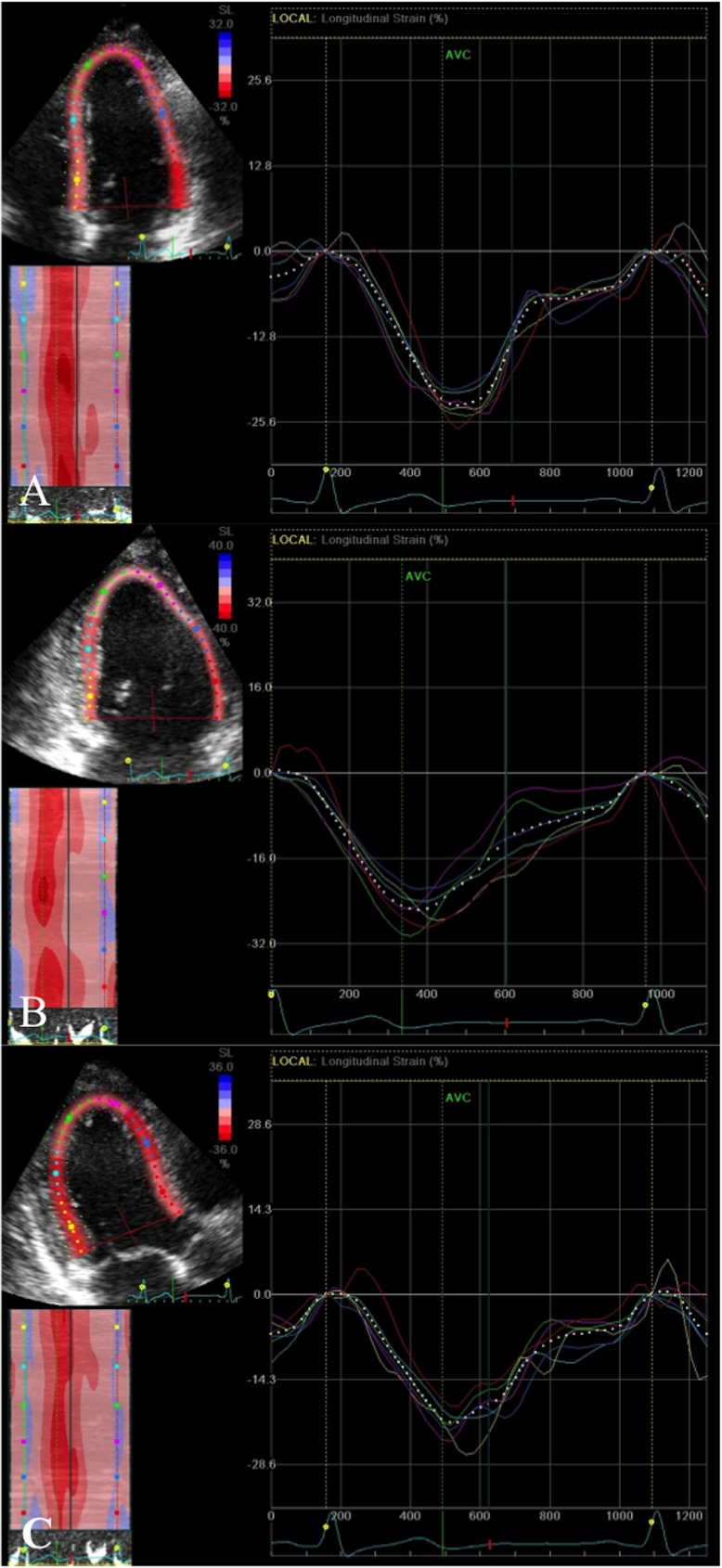
Aims: 2 dimensional (2D) strain analysis detects subclinical left ventricular (LV) systolic dysfunction. Our aim was to evaluate changes in LV systolic and diastolic function in breast cancer patients early after anthracycline chemotherapy, and to identify predisposing factors.
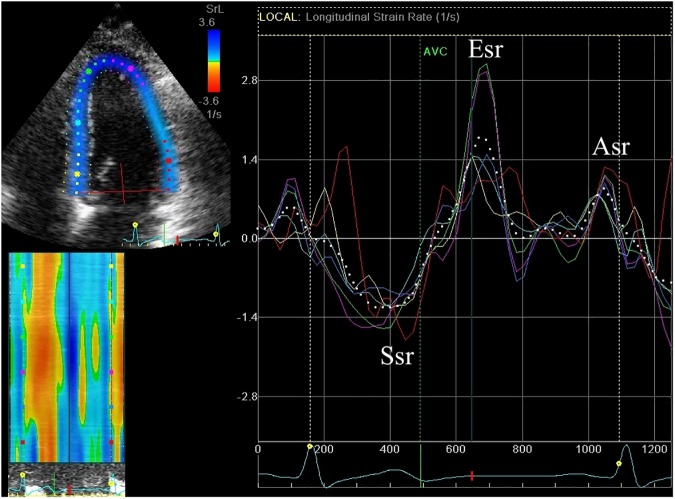
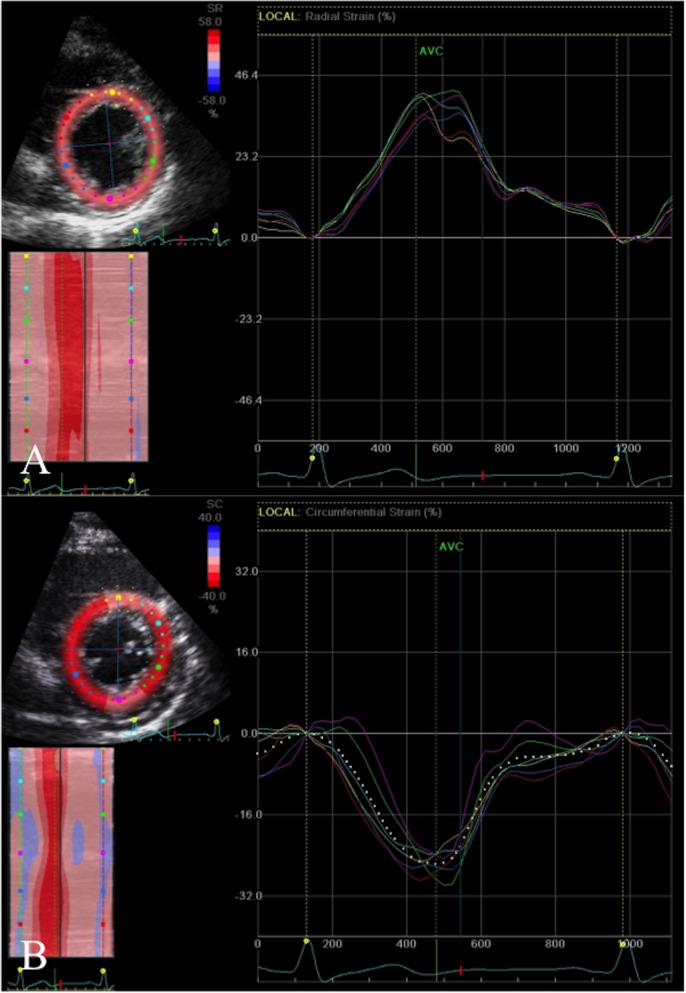
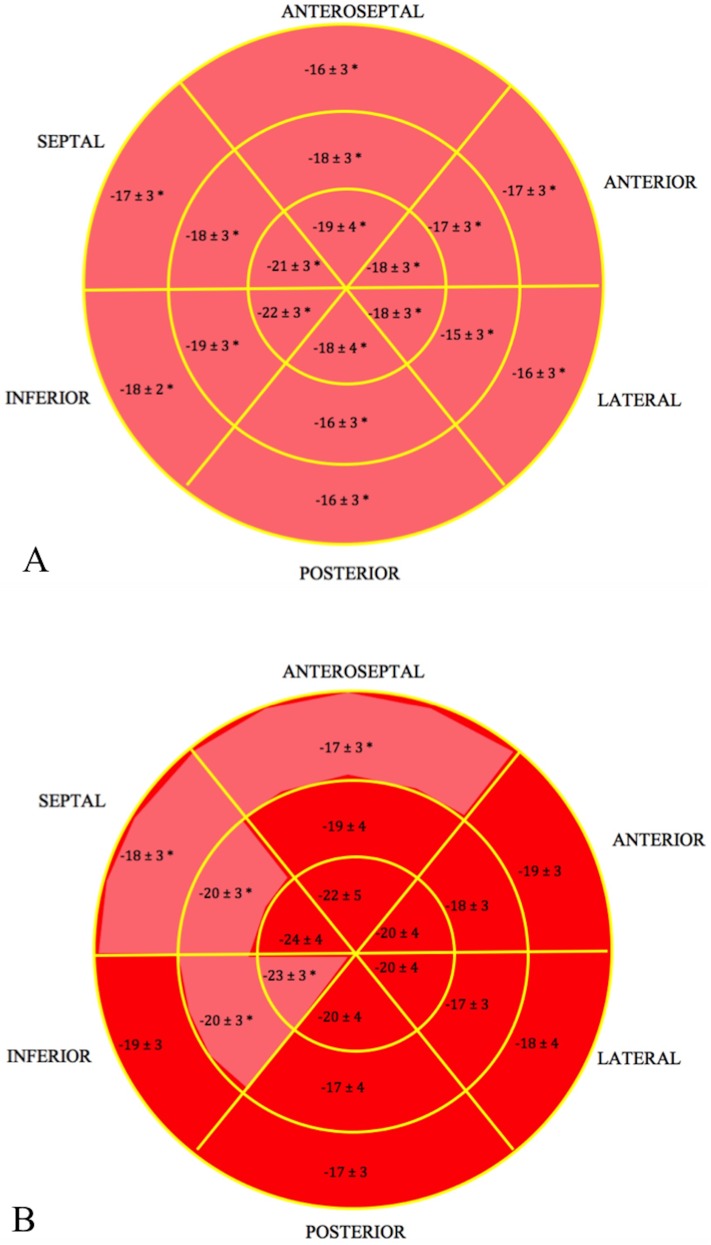
Methods and results: 140 patients were assessed by detailed echocardiography before and within seven days post treatment. LV ejection fraction (LVEF), global longitudinal strain (GLS), strain rate and radial and circumferential strain were assessed. Additionally, left atrial volumes and LV diastolic parameters were evaluated. LVEF although reduced after treatment, remained within the normal range (60±3% vs. 59±3%, p = 0.04). Triplane GLS was significantly reduced after treatment (-20.0±1.6% vs. -19.1±1.8%, p<0.001). Subclinical LV dysfunction (>11% reduction in GLS compared to before therapy) occurred in 22% (29/135). Impaired diastolic function grade significantly increased from 46% to 57% (p<0.001) after treatment. Furthermore, diastolic dysfunction was more common in the subgroup group with reduced systolic GLS compared to those without changes in GLS (30% vs. 11%; p = 0.04). No risk factors or clinical parameters were associated with the development of subclinical LV dysfunction; however the percentage change in early diastolic strain rate and the E velocity were independent predictors of >11% reduction in GLS.
Conclusion: Twenty two percent of patients had subclinical LV dysfunction by GLS, whilst none had cardiotoxicity defined by LVEF, demonstrating that GLS is more sensitive for detection of subclinical LV systolic dysfunction immediately after anthracycline therapy. Diastolic dysfunction increased, particularly in the group with reduced GLS, demonstrating the close pathophysiological relationship between systolic and diastolic function.
Conflict of interest statement
Figures
References
-
- Gianni L, Norton L, Wolmark N, Suter TM, Bonadonna G, Hortobagyi GN. Role of anthracyclines in the treatment of early breast cancer. J Clin Oncol. 2009;27: 4798–4808. doi: 10.1200/JCO.2008.21.4791 - DOI - PubMed
-
- Khasraw M, Bell R, Dang C. Epirubicin: Is it like doxorubicin in breast cancer? A clinical review. Breast. 2012;21: 142–149. doi: 10.1016/j.breast.2011.12.012 - DOI - PubMed
-
- Gianni L, Herman EH, Lipshultz SE, Minotti G, Sarvazyan N, Sawyer DB. Anthracycline cardiotoxicity: From bench to bedside. J Clin Oncol. 2008;26: 3777–3784. doi: 10.1200/JCO.2007.14.9401 - DOI - PMC - PubMed
-
- Khouri MG, Douglas PS, Mackey JR, Martin M, Scott JM, Scherrer-Crosbie M, et al. Cancer therapy-induced cardiac toxicity in early breast cancer: Addressing the unresolved issues. Circulation. 2012;126: 2749–2763. doi: 10.1161/CIRCULATIONAHA.112.100560 - DOI - PMC - PubMed
-
- Thavendiranathan P, Abdel-Qadir H, Fischer HD, Camacho X, Amir E, Austin PC, et al. Breast cancer therapy-related cardiac dysfunction in adult women treated in routine clinical practice: A population-based cohort study. J Clin Oncol. 2016;34: 2239–2246. doi: 10.1200/JCO.2015.65.1505 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
