

Complementary Features of Attention Bias Modification Therapy and Cognitive-Behavioral Therapy in Pediatric Anxiety Disorders
- PMID: 28407726
- PMCID: PMC6343478
- DOI: 10.1176/appi.ajp.2017.16070847
Complementary Features of Attention Bias Modification Therapy and Cognitive-Behavioral Therapy in Pediatric Anxiety Disorders
Erratum in
-
CORRECTION.Am J Psychiatry. 2018 Jan 1;175(1):83. doi: 10.1176/appi.ajp.2017.1751correction. Am J Psychiatry. 2018. PMID: 29301429 No abstract available.
Abstract
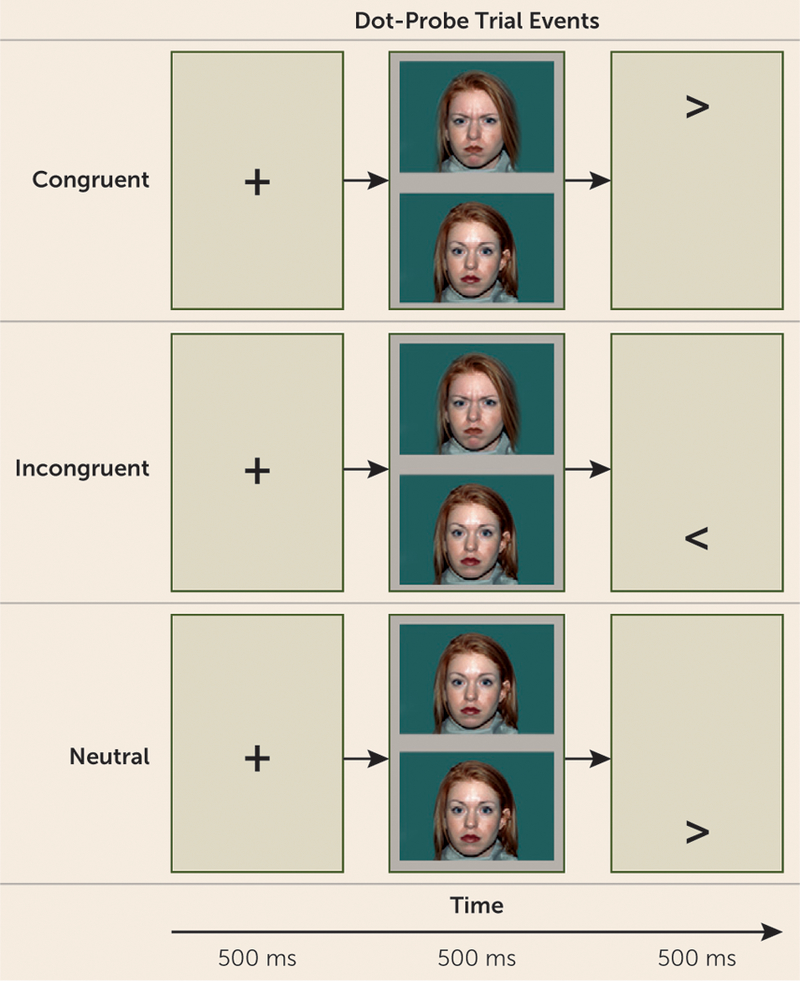
Objective: In the treatment of anxiety disorders, attention bias modification therapy (ABMT) and cognitive-behavioral therapy (CBT) may have complementary effects by targeting different aspects of perturbed threat responses and behaviors. ABMT may target rapid, implicit threat reactions, whereas CBT may target slowly deployed threat responses. The authors used amygdala-based connectivity during a threat-attention task and a randomized controlled trial design to evaluate potential complementary features of these treatments in pediatric anxiety disorders.
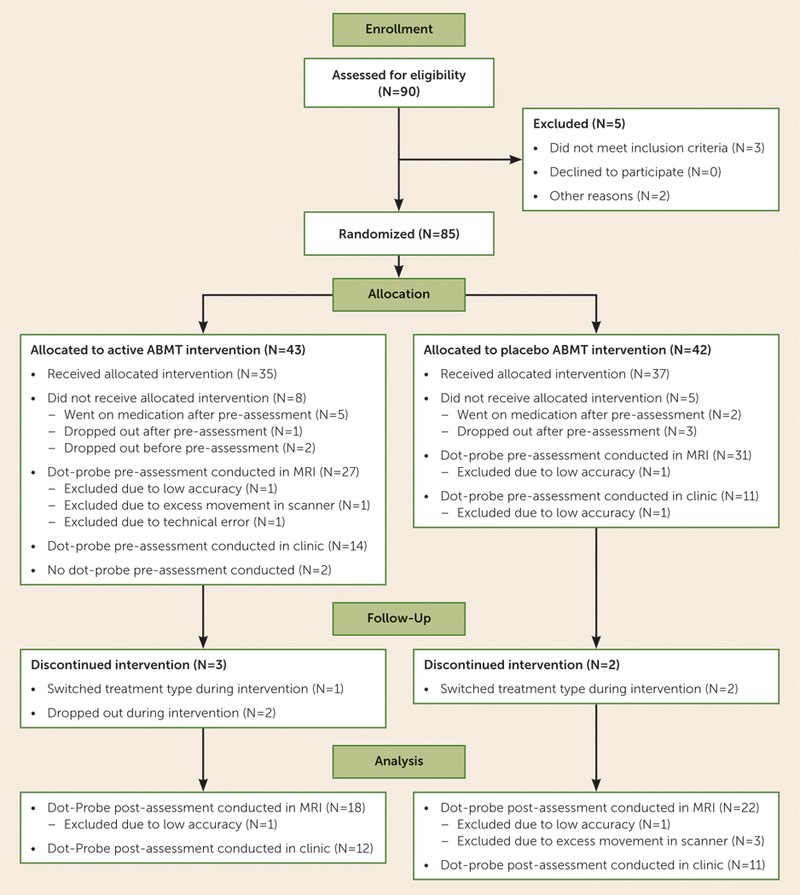
Method: Prior to treatment, youths (8-17 years old) with anxiety disorders (N=54), as well as healthy comparison youths (N=51), performed a threat-attention task during functional MRI acquisition. Task-related amygdala-based functional connectivity was assessed. Patients with and without imaging data (N=85) were then randomly assigned to receive CBT paired with either active or placebo ABMT. Clinical response was evaluated, and pretreatment amygdala-based connectivity profiles were compared among patients with varying levels of clinical response.
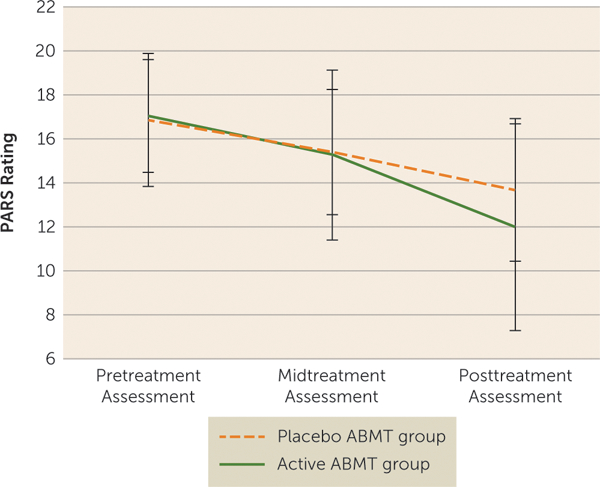
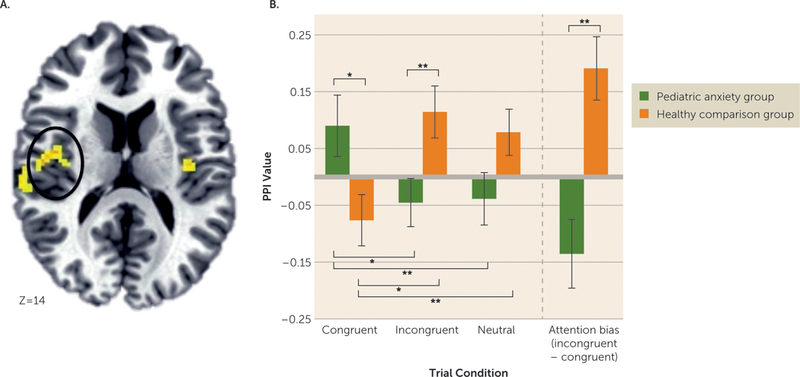
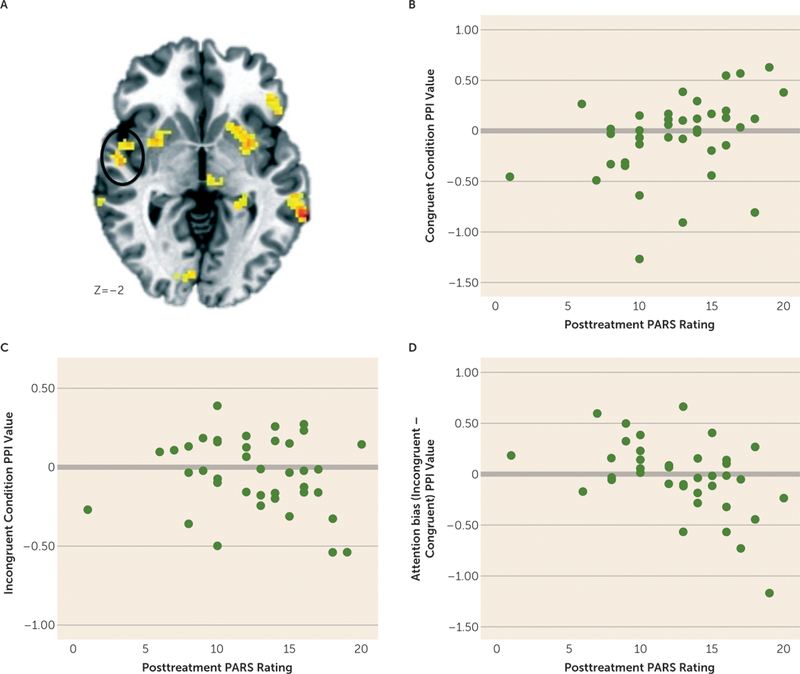
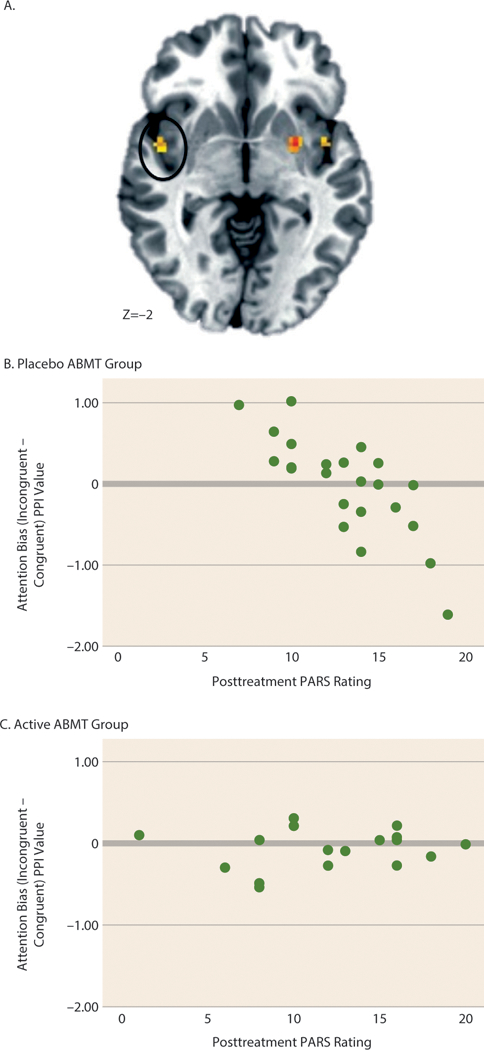
Results: Compared with the CBT plus placebo ABMT group, the CBT plus active ABMT group exhibited less severe anxiety after treatment. The patient and healthy comparison groups differed in amygdala-insula connectivity during the threat-attention task. Patients whose connectivity profiles were most different from those of the healthy comparison group exhibited the poorest response to treatment, particularly those who received CBT plus placebo ABMT.
Conclusions: The study provides evidence of enhanced clinical effects for patients receiving active ABMT. Moreover, ABMT appears to be most effective for patients with abnormal amygdala-insula connectivity. ABMT may target specific threat processes associated with dysfunctional amygdala-insula connectivity that are not targeted by CBT alone. This may explain the observation of enhanced clinical response to CBT plus active ABMT.
Trial registration: ClinicalTrials.gov NCT00018057.
Keywords: Adolescents; Anxiety Disorders; Attention Bias Modification; Child Psychiatry; Cognitive Neuroscience.
Conflict of interest statement
The authors report no financial relationships with commercial interests.
Figures
Comment in
-
Treatment of Anxiety Disorders in Youths: Filling the Cup Further.Am J Psychiatry. 2017 Aug 1;174(8):723-724. doi: 10.1176/appi.ajp.2017.17050544. Am J Psychiatry. 2017. PMID: 28760023 No abstract available.
References
-
- Bar-Haim Y, Lamy D, Pergamin L, et al. : Threat-related attentional bias in anxious and nonanxious individuals: a meta-analytic study. Psychol Bull 2007; 133:1–24 - PubMed
-
- Waters AM, Mogg K, Bradley BP, et al. : Attentionalbias for emotional faces in children with generalized anxiety disorder. J Am Acad Child Adolesc Psychiatry 2008; 47:435–442 - PubMed
-
- Pergamin-Hight L, Pine DS, Fox NA, et al. : Attention bias modification for youth with social anxiety disorder. J Child Psychol Psychiatry 2016; 57:1317–1325 - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
