

New drugs, new toxicities: severe side effects of modern targeted and immunotherapy of cancer and their management
- PMID: 28407743
- PMCID: PMC5391608
- DOI: 10.1186/s13054-017-1678-1
New drugs, new toxicities: severe side effects of modern targeted and immunotherapy of cancer and their management
Abstract
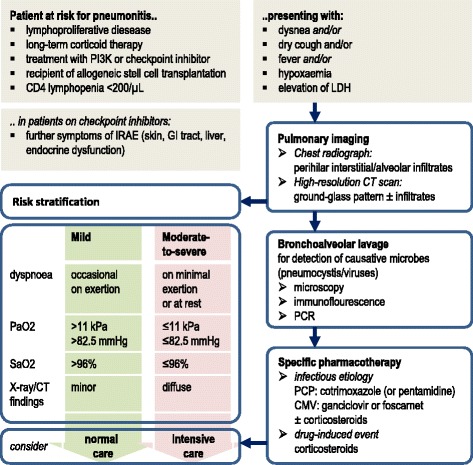
Pharmacological and cellular treatment of cancer is changing dramatically with benefits for patient outcome and comfort, but also with new toxicity profiles. The majority of adverse events can be classified as mild or moderate, but severe and life-threatening complications requiring ICU admission also occur. This review will focus on pathophysiology, symptoms, and management of these events based on the available literature.While standard antineoplastic therapy is associated with immunosuppression and infections, some of the recent approaches induce overwhelming inflammation and autoimmunity. Cytokine-release syndrome (CRS) describes a complex of symptoms including fever, hypotension, and skin reactions as well as lab abnormalities. CRS may occur after the infusion of monoclonal or bispecific antibodies (MABs, BABs) targeting immune effectors and tumor cells and is a major concern in recipients of chimeric antigen receptor (CAR) modified T lymphocytes as well. BAB and CAR T-cell treatment may also be compromised by central nervous system (CNS) toxicities such as encephalopathy, cerebellar alteration, disturbed consciousness, or seizures. While CRS is known to be induced by exceedingly high levels of inflammatory cytokines, the pathophysiology of CNS events is still unclear. Treatment with antibodies against inhibiting immune checkpoints can lead to immune-related adverse events (IRAEs); colitis, diarrhea, and endocrine disorders are often the cause for ICU admissions.Respiratory distress is the main reason for ICU treatment in cancer patients and is attributable to infectious agents in most cases. In addition, some of the new drugs are reported to cause non-infectious lung complications. While drug-induced interstitial pneumonitis was observed in a substantial number of patients treated with phosphoinositol-3-kinase inhibitors, IRAEs may also affect the lungs.Inhibitors of angiogenetic pathways have increased the antineoplastic portfolio. However, vessel formation is also essential for regeneration and tissue repair. Therefore, severe vascular side effects, including thromboembolic events, gastrointestinal bleeding or perforation, hypertension, and congestive heart failure, compromise antitumor efficacy.The limited knowledge of the pathophysiology and management of life-threatening complications relating to new cancer drugs presents a need to provide ICU staff, oncologists, and organ specialists with evidence-based algorithms.
Keywords: Cancer; Immunotherapy; Interdisciplinary management; Targeted therapy; Toxicity.
Figures

References
-
- Kunkel L, Wong A, Maneatis T, Nickas J, Brown T, Grillo-López A, Benyunes M, Grobman B, Dillman RO. Optimizing the use of rituximab for treatment of B-cell non-Hodgkin's lymphoma: a benefit-risk update. Semin Oncol. 2000;27(6 Suppl 12):53–61. - PubMed
-
- Coiffier B, Lepretre S, Pedersen LM, Gadeberg O, Fredriksen H, van Oers MHJ, Wooldridge J, Kloczko J, Holowiecki J, Hellmann A, Walewski J, Flensburg M, Petersen J, Robak T. Safety and efficacy of ofatumumab, a fully human monoclonal anti-CD20 antibody, in patients with relapsed or refractory B-cell chronic lymphocytic leukemia: a phase 1-2 study. Blood. 2008;111:1094–1100. doi: 10.1182/blood-2007-09-111781. - DOI - PubMed
-
- Goede V, Fischer K, Busch R, Engelke A, Eichhorst B, Wendtner CM, Chagorova T, de la Serna J, Dilhuydy MS, Illmer T, Opat S, Owen CJ, Samoylova O, Kreuzer KA, Stilgenbauer S, Döhner H, Langerak AW, Ritgen M, Kneba M, Asikanius E, Humphrey K, Wenger M, Hallek M. Obinutuzumab plus chlorambucil in patients with CLL and coexisting conditions. N Engl J Med. 2014;370(12):1101–1110. doi: 10.1056/NEJMoa1313984. - DOI - PubMed
-
- Van Cutsem E, Köhne CH, Hitre E, Zaluski J, Chang Chien CR, Makhson A, D'Haens G, Pintér T, Lim R, Bodoky G, Roh JK, Folprecht G, Ruff P, Stroh C, Tejpar S, Schlichting M, Nippgen J, Rougier P. Cetuximab and chemotherapy as initial treatment for metastatic colorectal cancer. N Engl J Med. 2009;360(14):1408–1417. doi: 10.1056/NEJMoa0805019. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
