

A study of noninvasive fractional flow reserve derived from a simplified method based on coronary computed tomography angiography in suspected coronary artery disease
- PMID: 28407768
- PMCID: PMC5391576
- DOI: 10.1186/s12938-017-0330-2
A study of noninvasive fractional flow reserve derived from a simplified method based on coronary computed tomography angiography in suspected coronary artery disease
Abstract
Background: The invasive fractional flow reserve has been considered the gold standard for identifying ischaemia-related stenosis in patients with suspected coronary artery disease. Determining non-invasive FFR based on coronary computed tomographic angiography datasets using computational fluid dynamics tends to be a demanding process. Therefore, the diagnostic performance of a simplified method for the calculation of FFRCTA requires further evaluation.
Objectives: The aim of this study was to investigate the diagnostic performance of FFRCTA calculated based on a simplified method by referring to the invasive FFR in patient-specific coronary arteries and clinical decision-making.
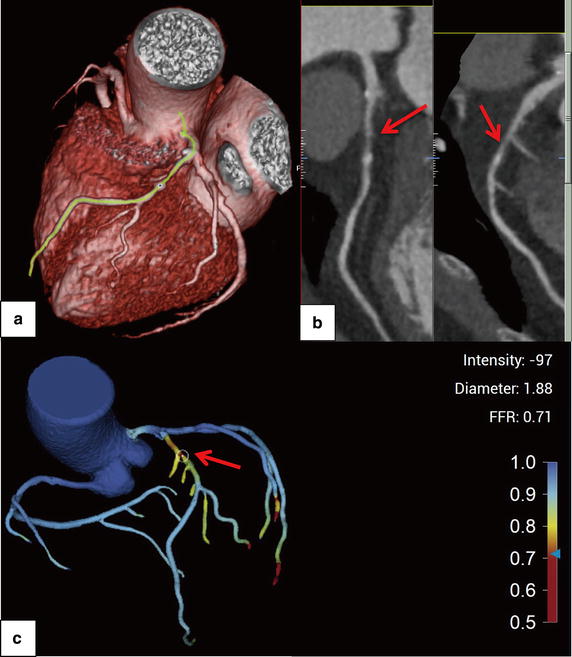
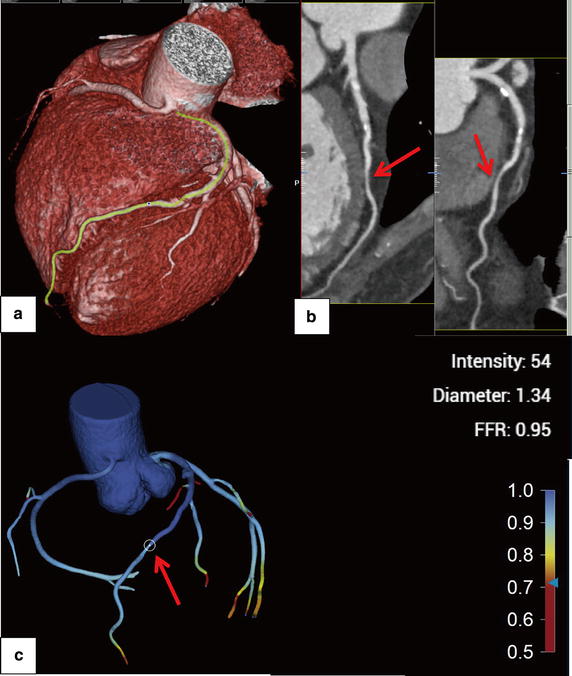
Methods: Twenty-nine subjects included in this study underwent CCTA before undergoing clinically indicated invasive coronary angiography for suspected coronary artery disease. Pulsatile flow simulation and a novel boundary condition were used to obtain FFRCTA based on the CCTA datasets. The Pearson correlation, Bland-Altman plots and the diagnostic performance of FFRCTA and CCTA stenosis were analyzed by comparison to the invasive FFR reference standard. Ischaemia was defined as an FFR or FFRCTA ≤0.80, and anatomically obstructive CAD was defined as a CCTA stenosis >50%.
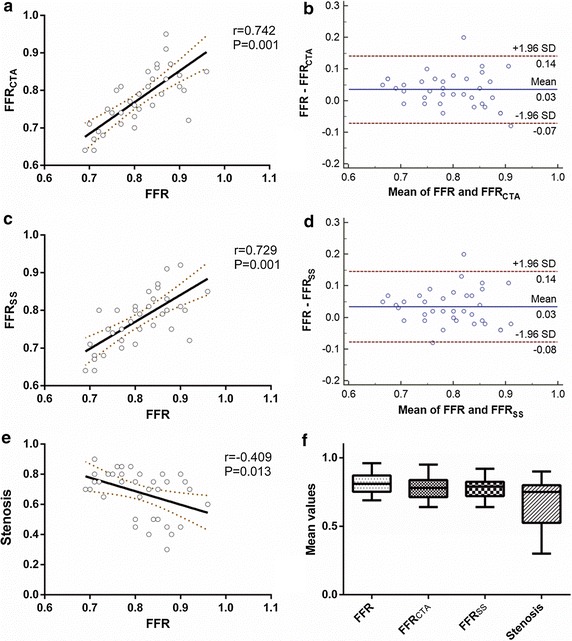
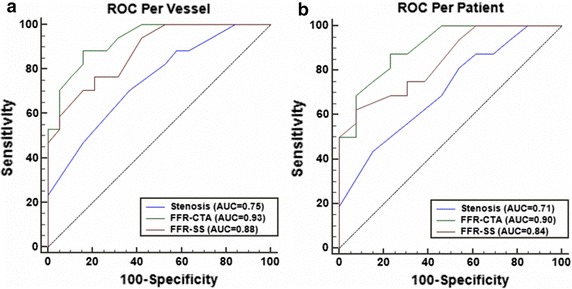
Results: FFRCTA and invasive FFR were well correlated (r = 0.742, P = 0.001). Slight systematic underestimation was found in FFRCTA (mean difference 0.03, standard deviation 0.05, P = 0.001). The area under the receiver-operating characteristic curve was 0.93 for FFRCTA and 0.75 for CCTA on a per-vessel basis. Per-patient accuracy, sensitivity and specificity were 79.3, 93.7 and 61.5%, respectively, for FFRCTA and 62.1, 87.5 and 30.7%, respectively, for CCTA. Per-vessel accuracy, sensitivity and specificity were 80.6, 94.1 and 68.4%, respectively, for FFRCTA and 61.6, 88.2 and 36.8%, respectively, for CCTA.
Conclusions: FFRCTA derived from pulsatile simulation with a simplified novel boundary condition was in good agreement with invasive FFR and showed better diagnostic performance compared to CCTA, suggesting that the simplified method has the potential to be an alternative and accurate way to assess the haemodynamic characteristics for coronary stenosis.
Keywords: CCTA; CFD; FFR; FFRCTA.
Figures
References
-
- Shaw LJ, et al. Optimal medical therapy with or without percutaneous coronary intervention to reduce ischemic burden: results from the Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation (COURAGE) trial nuclear substudy. Circulation. 2008;117(10):1283–1291. doi: 10.1161/CIRCULATIONAHA.107.743963. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
