

The Diagnosis of Urinary Tract Infection in Young Children (DUTY) Study Clinical Rule: Economic Evaluation
- PMID: 28407997
- PMCID: PMC5406157
- DOI: 10.1016/j.jval.2017.01.003
The Diagnosis of Urinary Tract Infection in Young Children (DUTY) Study Clinical Rule: Economic Evaluation
Abstract
Objective: To estimate the cost-effectiveness of a two-step clinical rule using symptoms, signs and dipstick testing to guide the diagnosis and antibiotic treatment of urinary tract infection (UTI) in acutely unwell young children presenting to primary care.
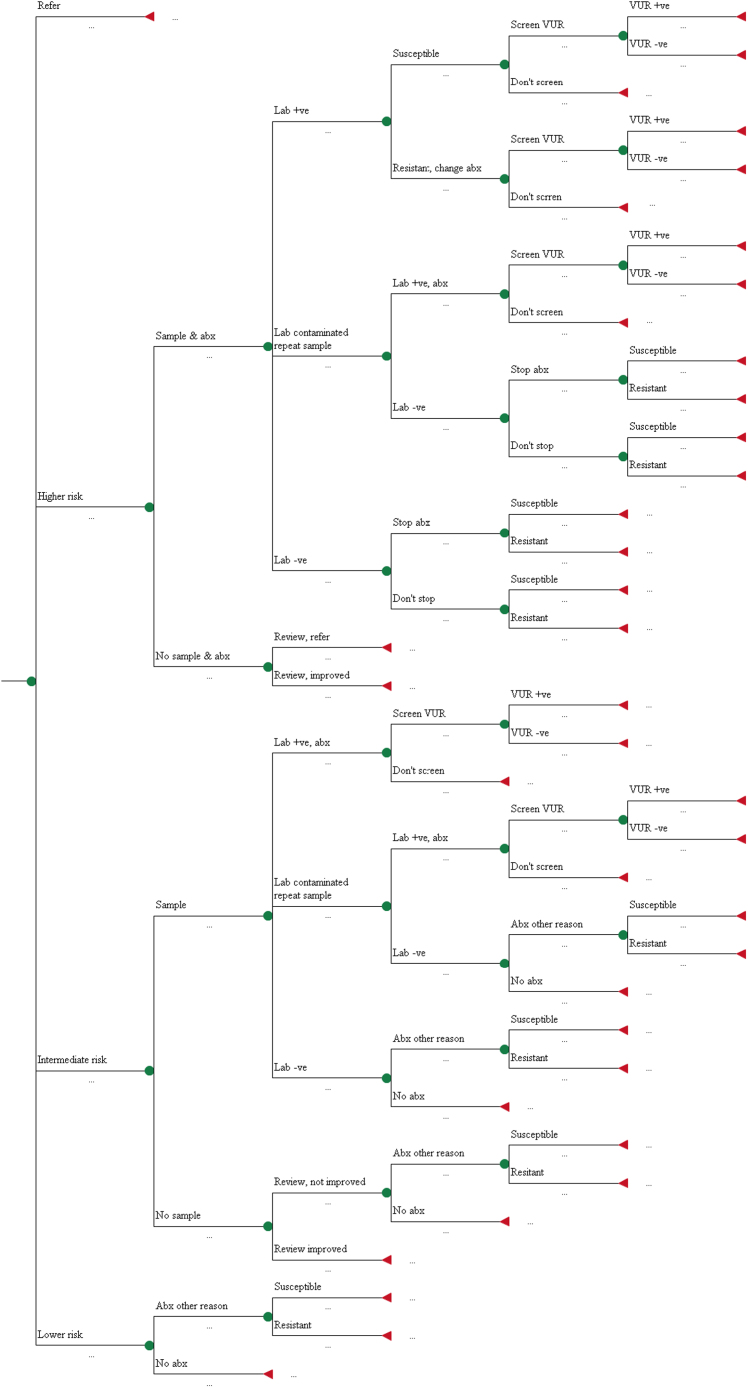
Methods: Decision analytic model synthesising data from a multicentre, prospective cohort study (DUTY) and the wider literature to estimate the short-term and lifetime costs and healthcare outcomes (symptomatic days, recurrent UTI, quality adjusted life years) of eight diagnostic strategies. We compared GP clinical judgement with three strategies based on a 'coefficient score' combining seven symptoms and signs independently associated with UTI and four strategies based on weighted scores according to the presence/absence of five symptoms and signs. We compared dipstick testing versus laboratory culture in children at intermediate risk of UTI.
Results: Sampling, culture and antibiotic costs were lowest in high-specificity DUTY strategies (£1.22 and £1.08) compared to clinical judgement (£1.99). These strategies also approximately halved urine sampling (4.8% versus 9.1% in clinical judgement) without reducing sensitivity (58.2% versus 56.4%). Outcomes were very similar across all diagnostic strategies. High-specificity DUTY strategies were more cost-effective than clinical judgement in the short- (iNMB = £0.78 and £0.84) and long-term (iNMB =£2.31 and £2.50). Dipstick tests had poorer cost-effectiveness than laboratory culture in children at intermediate risk of UTI (iNMB = £-1.41).
Conclusions: Compared to GPs' clinical judgement, high specificity clinical rules from the DUTY study could substantially reduce urine sampling, achieving lower costs and equivalent patient outcomes. Dipstick testing children for UTI is not cost-effective.
Keywords: antibacterial agents; diagnosis; economics; medical; pediatrics; urinary tract infections.
Copyright © 2017 International Society for Pharmacoeconomics and Outcomes Research (ISPOR). Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
The Diagnosis of Urinary Tract infection in Young children (DUTY): a diagnostic prospective observational study to derive and validate a clinical algorithm for the diagnosis of urinary tract infection in children presenting to primary care with an acute illness.Health Technol Assess. 2016 Jul;20(51):1-294. doi: 10.3310/hta20510. Health Technol Assess. 2016. PMID: 27401902 Free PMC article.
-
Dipsticks and diagnostic algorithms in urinary tract infection: development and validation, randomised trial, economic analysis, observational cohort and qualitative study.Health Technol Assess. 2009 Mar;13(19):iii-iv, ix-xi, 1-73. doi: 10.3310/hta13190. Health Technol Assess. 2009. PMID: 19364448 Review.
-
Improving the Diagnosis and Treatment of Urinary Tract Infection in Young Children in Primary Care: Results from the DUTY Prospective Diagnostic Cohort Study.Ann Fam Med. 2016 Jul;14(4):325-36. doi: 10.1370/afm.1954. Ann Fam Med. 2016. PMID: 27401420 Free PMC article.
-
Vesicoureteral Reflux.2024 Apr 30. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2024 Apr 30. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 33085409 Free Books & Documents.
-
Urinary tract infections in multiple sclerosis.Mult Scler. 2016 Jun;22(7):855-61. doi: 10.1177/1352458516633903. Epub 2016 Feb 18. Mult Scler. 2016. PMID: 26892318 Review.
Cited by
-
Availability and use of rapid diagnostic tests for the management of acute childhood infections in Europe: A cross-sectional survey of paediatricians.PLoS One. 2022 Dec 20;17(12):e0275336. doi: 10.1371/journal.pone.0275336. eCollection 2022. PLoS One. 2022. PMID: 36538525 Free PMC article.
-
Clinical prediction rules for childhood urinary tract infections: a cross-sectional study in ambulatory care.BJGP Open. 2022 Aug 30;6(2):BJGPO.2021.0171. doi: 10.3399/BJGPO.2021.0171. Print 2022 Jun. BJGP Open. 2022. PMID: 35031560 Free PMC article.
-
Improving event prediction using general practitioner clinical judgement in a digital risk stratification model: a pilot study.BMC Med Inform Decis Mak. 2024 Dec 18;24(1):382. doi: 10.1186/s12911-024-02797-5. BMC Med Inform Decis Mak. 2024. PMID: 39696351 Free PMC article.
-
Long-term outcomes of urinary tract infection (UTI) in Childhood (LUCI): protocol for an electronic record-linked cohort study.BMJ Open. 2019 Apr 20;9(4):e024210. doi: 10.1136/bmjopen-2018-024210. BMJ Open. 2019. PMID: 31005909 Free PMC article.
-
Urine collection methods and dipstick testing in non-toilet-trained children.Pediatr Nephrol. 2021 Jul;36(7):1697-1708. doi: 10.1007/s00467-020-04742-w. Epub 2020 Sep 12. Pediatr Nephrol. 2021. PMID: 32918601 Free PMC article. Review.
References
-
- Petersen I., Hayward A.C., Sacar Surveillance Subgroup Antibacterial prescribing in primary care. J Antimicrob Chemother. 2007;60(Suppl. 1):i43–i47. - PubMed
-
- Whiting P., Westwood M., Bojke L. Clinical effectiveness and cost-effectiveness of tests for the diagnosis and investigation of urinary tract infection in children: a systematic review and economic model. Health Technol Assess. 2006;10:1–154. - PubMed
-
- National Institute for Health and Clinical Excellence . National Institute for Health and Clinical Excellence; London: 2007. Urinary Tract Infection in Children: Diagnosis, Treatment and Long Term Management.
-
- Smith R., Coast J. The true cost of antimicrobial resistance. BMJ. 2013;346:f1493. - PubMed
-
- Downs S.M. Technical report: urinary tract infections in febrile infants and young children. The Urinary Tract Subcommittee of the American Academy of Pediatrics Committee on Quality Improvement. Pediatrics. 1999;103:e54. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
