

Apolipoprotein(a) isoform size, lipoprotein(a) concentration, and coronary artery disease: a mendelian randomisation analysis
- PMID: 28408323
- PMCID: PMC5483508
- DOI: 10.1016/S2213-8587(17)30088-8
Apolipoprotein(a) isoform size, lipoprotein(a) concentration, and coronary artery disease: a mendelian randomisation analysis
Erratum in
-
Correction to Lancet Diabetes Endocrinol 2017; 5: 524-33.Lancet Diabetes Endocrinol. 2017 Sep;5(9):e6. doi: 10.1016/S2213-8587(17)30267-X. Lancet Diabetes Endocrinol. 2017. PMID: 28842162 Free PMC article. No abstract available.
Abstract
Background: The lipoprotein(a) pathway is a causal factor in coronary heart disease. We used a genetic approach to distinguish the relevance of two distinct components of this pathway, apolipoprotein(a) isoform size and circulating lipoprotein(a) concentration, to coronary heart disease.
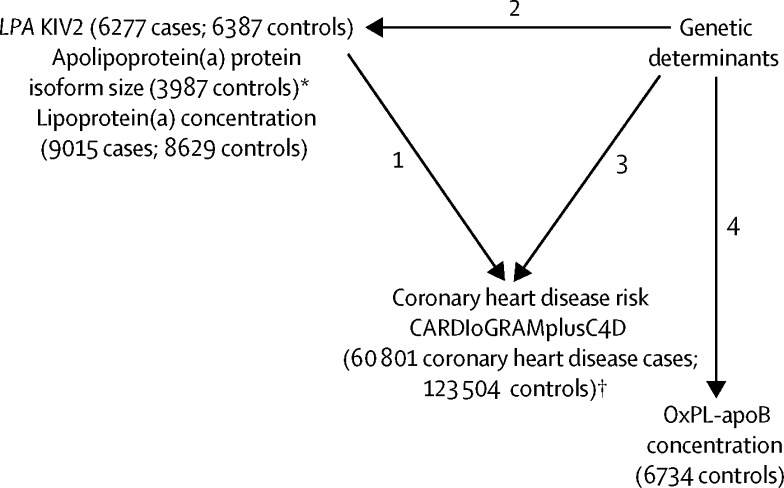
Methods: In this mendelian randomisation study, we measured lipoprotein(a) concentration and determined apolipoprotein(a) isoform size with a genetic method (kringle IV type 2 [KIV2] repeats in the LPA gene) and a serum-based electrophoretic assay in patients and controls (frequency matched for age and sex) from the Pakistan Risk of Myocardial Infarction Study (PROMIS). We calculated odds ratios (ORs) for myocardial infarction per 1-SD difference in either LPA KIV2 repeats or lipoprotein(a) concentration. In a genome-wide analysis of up to 17 503 participants in PROMIS, we identified genetic variants associated with either apolipoprotein(a) isoform size or lipoprotein(a) concentration. Using a mendelian randomisation study design and genetic data on 60 801 patients with coronary heart disease and 123 504 controls from the CARDIoGRAMplusC4D consortium, we calculated ORs for myocardial infarction with variants that produced similar differences in either apolipoprotein(a) isoform size in serum or lipoprotein(a) concentration. Finally, we compared phenotypic versus genotypic ORs to estimate whether apolipoprotein(a) isoform size, lipoprotein(a) concentration, or both were causally associated with coronary heart disease.
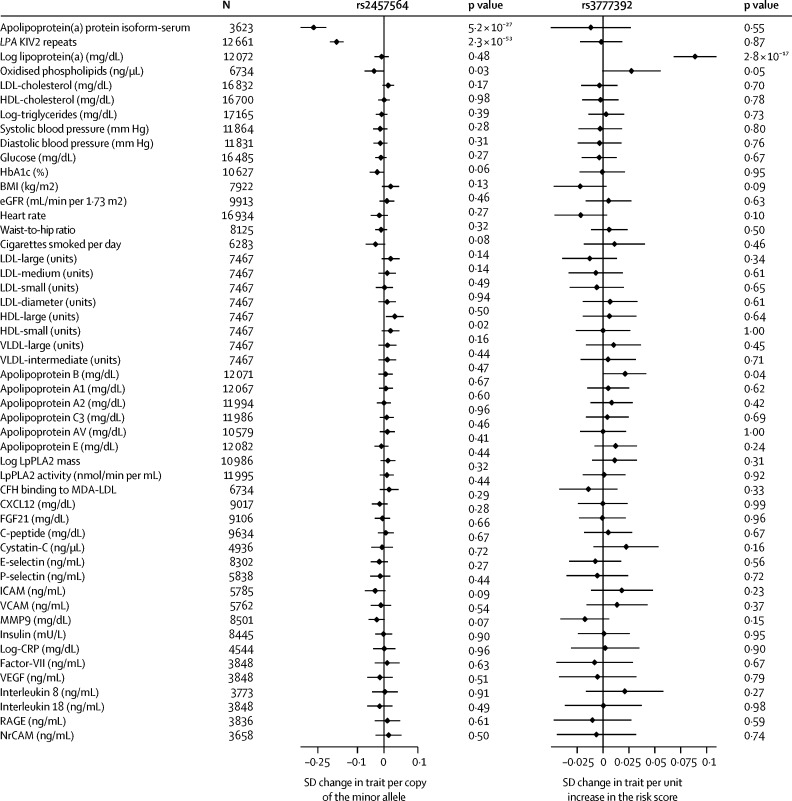
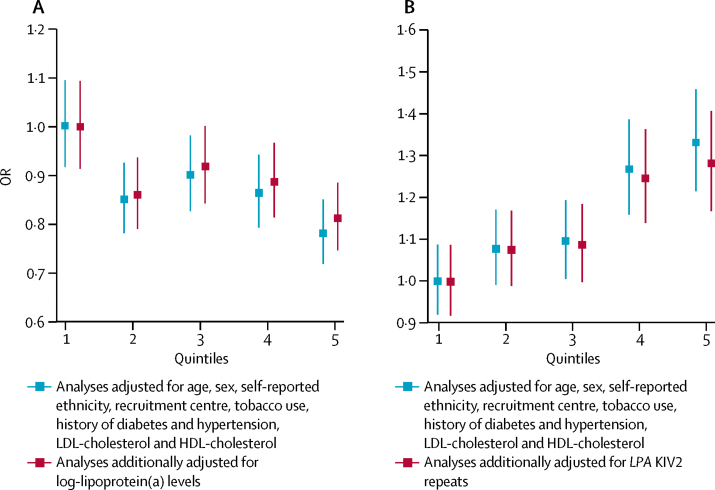
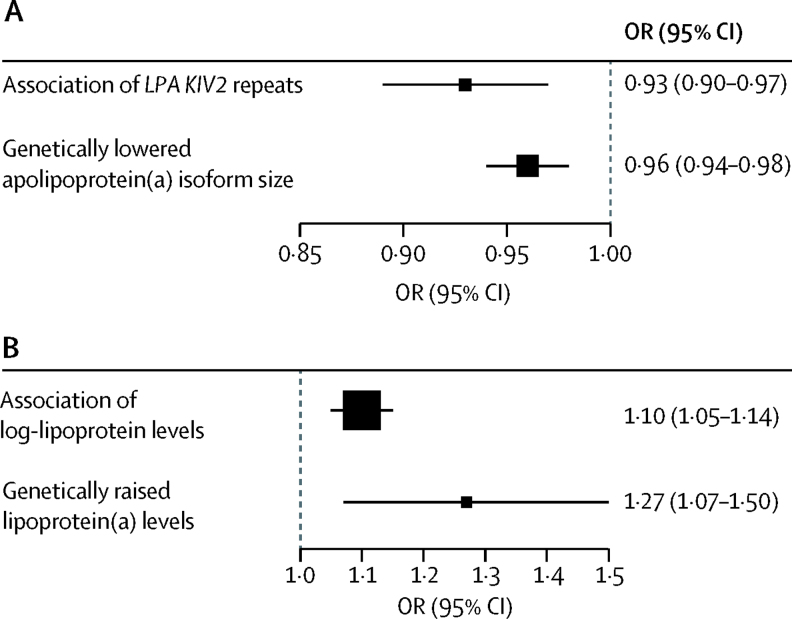
Findings: The PROMIS cohort included 9015 patients with acute myocardial infarction and 8629 matched controls. In participants for whom KIV2 repeat and lipoprotein(a) data were available, the OR for myocardial infarction was 0·93 (95% CI 0·90-0·97; p<0·0001) per 1-SD increment in LPA KIV2 repeats after adjustment for lipoprotein(a) concentration and conventional lipid concentrations. The OR for myocardial infarction was 1·10 (1·05-1·14; p<0·0001) per 1-SD increment in lipoprotein(a) concentration, after adjustment for LPA KIV2 repeats and conventional lipids. Genome-wide analysis identified rs2457564 as a variant associated with smaller apolipoprotein(a) isoform size, but not lipoprotein(a) concentration, and rs3777392 as a variant associated with lipoprotein(a) concentration, but not apolipoprotein(a) isoform size. In 60 801 patients with coronary heart disease and 123 504 controls, OR for myocardial infarction was 0·96 (0·94-0·98; p<0·0001) per 1-SD increment in apolipoprotein(a) protein isoform size in serum due to rs2457564, which was directionally concordant with the OR observed in PROMIS for a similar change. The OR for myocardial infarction was 1·27 (1·07-1·50; p=0·007) per 1-SD increment in lipoprotein(a) concentration due to rs3777392, which was directionally concordant with the OR observed for a similar change in PROMIS.
Interpretation: Human genetic data suggest that both smaller apolipoprotein(a) isoform size and increased lipoprotein(a) concentration are independent and causal risk factors for coronary heart disease. Lipoprotein(a)-lowering interventions could be preferentially effective in reducing the risk of coronary heart disease in individuals with smaller apolipoprotein(a) isoforms.
Funding: British Heart Foundation, US National Institutes of Health, Fogarty International Center, Wellcome Trust, UK Medical Research Council, UK National Institute for Health Research, and Pfizer.
Copyright © 2017 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
What role for lipoprotein(a) in clinical practice?Lancet Diabetes Endocrinol. 2017 Jul;5(7):487-489. doi: 10.1016/S2213-8587(17)30063-3. Epub 2017 Apr 10. Lancet Diabetes Endocrinol. 2017. PMID: 28408322 No abstract available.
References
-
- Clarke R, Peden JF, Hopewell JC. Genetic variants associated with Lp(a) lipoprotein level and coronary disease. N Engl J Med. 2009;361:2518–2528. - PubMed
-
- Erqou S, Thompson A, Di AE. Apolipoprotein(a) isoforms and the risk of vascular disease: systematic review of 40 studies involving 58,000 participants. J Am Coll Cardiol. 2010;55:2160–2167. - PubMed
-
- Kamstrup PR, Tybjaerg-Hansen A, Steffensen R, Nordestgaard BG. Genetically elevated lipoprotein(a) and increased risk of myocardial infarction. JAMA. 2009;301:2331–2339. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
