

A Host-Dependent Prognostic Model for Elderly Patients with Diffuse Large B-Cell Lymphoma
- PMID: 28408622
- PMCID: PMC5423505
- DOI: 10.1634/theoncologist.2016-0260
A Host-Dependent Prognostic Model for Elderly Patients with Diffuse Large B-Cell Lymphoma
Abstract
Background: Decision-making models for elderly patients with diffuse large B-cell lymphoma (DLBCL) treated with rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) are in great demand.
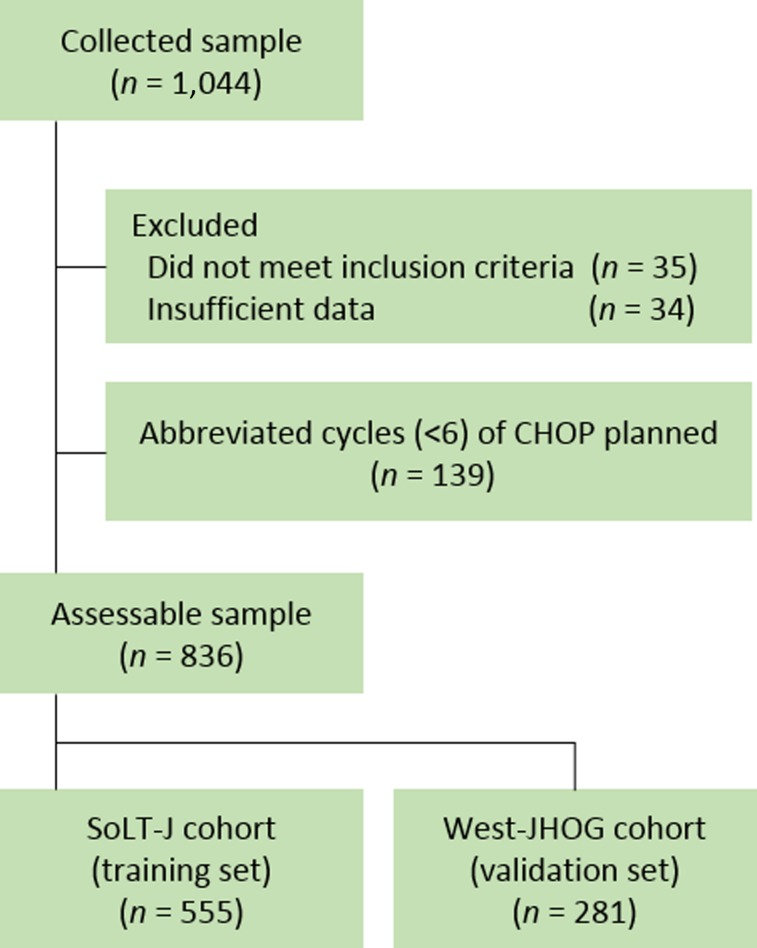
Patients and methods: The Society of Lymphoma Treatment in Japan (SoLT-J), in collaboration with the West-Japan Hematology and Oncology Group (West-JHOG), collected and retrospectively analyzed the clinical records of ≥65-year-old patients with DLBCL treated with R-CHOP from 19 sites across Japan to build an algorithm that can stratify adherence to R-CHOP.
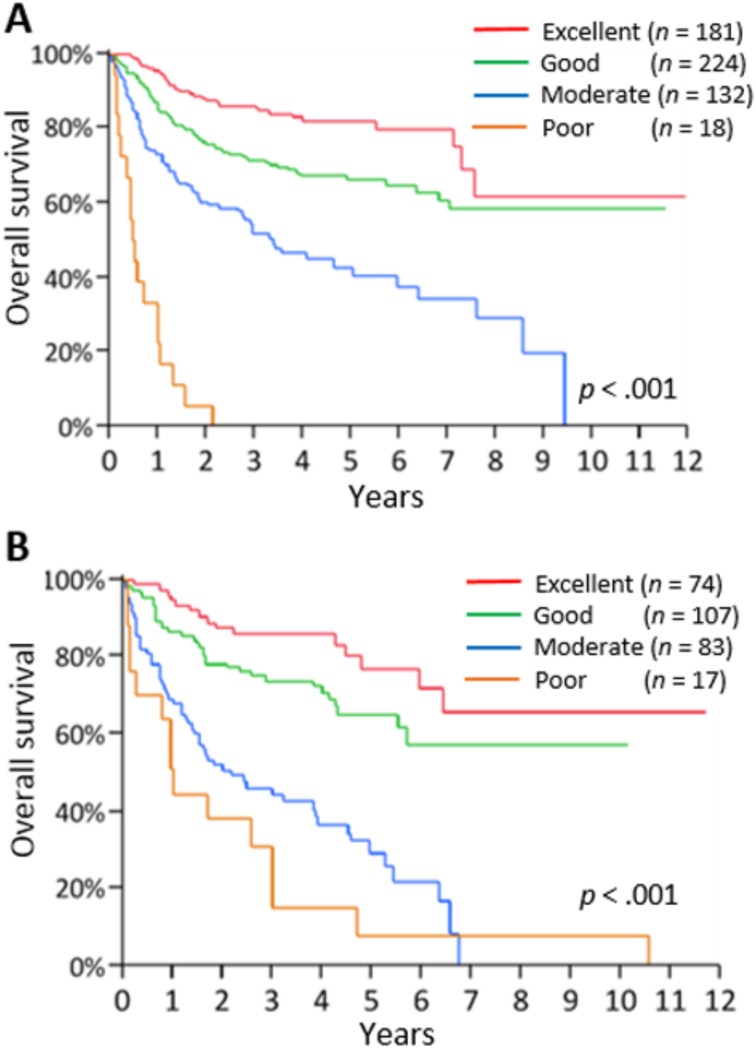
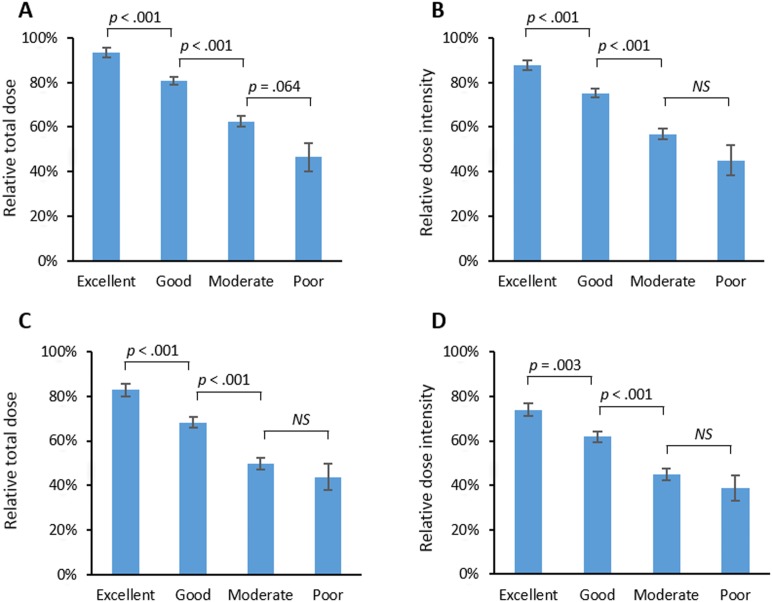
Results: A total of 836 patients with a median age of 74 years (range, 65-96 years) were analyzed. In the SoLT-J cohort (n = 555), age >75 years, serum albumin level <3.7 g/dL, and Charlson Comorbidity Index score ≥3 were independent adverse risk factors and were defined as the Age, Comorbidities, and Albumin (ACA) index. Based on their ACA index score, patients were categorized into "excellent" (0 points), "good" (1 point), "moderate" (2 points), and "poor" (3 points) groups. This grouping effectively discriminated the 3-year overall survival rates, mean relative total doses (or relative dose intensity) of anthracycline and cyclophosphamide, unanticipated R-CHOP discontinuance rates, febrile neutropenia rates, and treatment-related death rates. Additionally, the ACA index showed comparable results for these clinical parameters when it was applied to the West-JHOG cohort (n = 281).
Conclusion: The ACA index has the ability to stratify the prognosis, tolerability to cytotoxic drugs, and adherence to treatment of elderly patients with DLBCL treated with R-CHOP. The Oncologist 2017;22:554-560 IMPLICATIONS FOR PRACTICE: Currently, little is known regarding how to identify elderly patients with diffuse large B-cell lymphoma who may tolerate a full dose of chemotherapy or to what extent cytotoxic drugs should be reduced in some specific conditions. The Society of Lymphoma Treatment in Japan developed a host-dependent prognostic model consisting of higher age (>75 years), hypoalbuminemia (<3.7 g/dL), and higher Charlson Comorbidity Index score (≥3) for such elderly patients. This model can stratify the prognosis, tolerability to cytotoxic drugs, and adherence to treatment of these patients and thus help clinicians in formulating personalized treatment strategies for this growing patient population.
Keywords: Comorbidity; Diffuse large B‐cell lymphoma; Geriatric assessment; Hypoalbuminemia; Personalized medicine; R‐CHOP chemotherapy.
© AlphaMed Press 2017.
Conflict of interest statement
Disclosures of potential conflicts of interest may be found at the end of this article.
Figures
References
-
- A predictive model for aggressive non‐Hodgkin's lymphoma . The International Non‐Hodgkin's Lymphoma Prognostic Factors Project. N Engl J Med 1993;329:987–994. - PubMed
-
- Sehn LH, Berry B, Chhanabhai M et al. The revised International Prognostic Index (R‐IPI) is a better predictor of outcome than the standard IPI for patients with diffuse large B‐cell lymphoma treated with R‐CHOP. Blood 2007;109:1857–1861. - PubMed
-
- DeSantis CE, Lin CC, Mariotto AB et al. Cancer treatment and survivorship statistics, 2014. CA Cancer J Clin 2014;64:252–271. - PubMed
-
- Lichtman SM. Chemotherapy in the elderly. Semin Oncol 2004;31:160–174. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
