

Reliably estimating prevalences of atopic children: an epidemiological study in an extensive and representative primary care database
- PMID: 28408759
- PMCID: PMC5435092
- DOI: 10.1038/s41533-017-0025-y
Reliably estimating prevalences of atopic children: an epidemiological study in an extensive and representative primary care database
Abstract
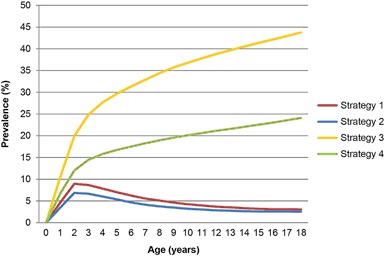
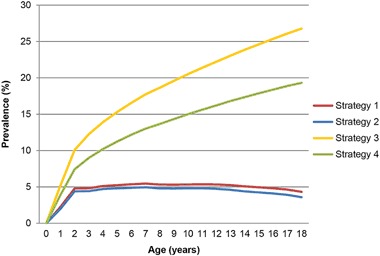
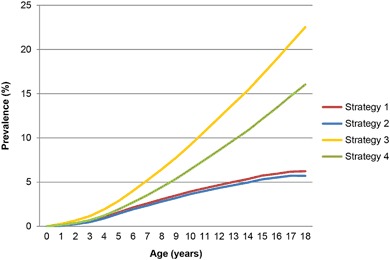
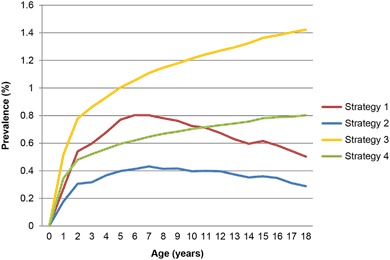
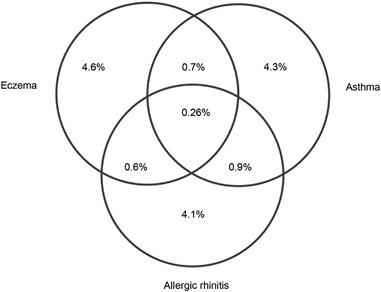
Electronic health records stored in primary care databases might be a valuable source to study the epidemiology of atopic disorders and their impact on health-care systems and costs. However, the prevalence of atopic disorders in such databases varies considerably and needs to be addressed. For this study, all children aged 0-18 years listed in a representative primary care database in the period 2002-2014, with sufficient data quality, were selected. The effects of four different strategies on the prevalences of atopic disorders were examined: (1) the first strategy examined the diagnosis as recorded in the electronic health records, whereas the (2) second used additional requirements (i.e., the patient had at least two relevant consultations and at least two relevant prescriptions). Strategies (3) and (4) assumed the atopic disorders to be chronic based on strategy 1 and 2, respectively. When interested in cases with a higher probability of a clinically relevant disorder, strategy 2 yields a realistic estimation of the prevalence of atopic disorders derived from primary care data. Using this strategy, of the 478,076 included children, 28,946 (6.1%) had eczema, 29,182 (6.1%) had asthma, and 28,064 (5.9%) had allergic rhinitis; only 1251 (0.3%) children had all three atopic disorders. Prevalence rates are highly dependent on the clinical atopic definitions used. The strategy using cases with a higher probability of clinically relevant cases, yields realistic prevalences to establish the impact of atopic disorders on health-care systems. However, studies are needed to solve the problem of identifying atopic disorders that are missed or misclassified.
Atopic disorders: CLINICAL INFORMATION IMPROVES PREVALENCE ESTIMATES: The prevalence of atopic disorders in children can be more reliably calculated by incorporating clinical information with diagnosis data. Researchers in the Netherlands, led by David Pols from the Erasmus University Medical Center Rotterdam, examined the electronic health records of more than 660,000 children, aged 0 to 18, from a Dutch primary care database to determine the number of cases of atopic eczema, asthma, and allergic rhinitis. They looked for diagnosed children who also had at least two relevant clinical consultations and at least two relevant prescriptions. This strategy helps correct for the problem of overestimation, because it doesnot assume that a child, once diagnosed, will have an atopic disorder for life. However, other methods are still needed to identify cases that are missed or misclassified in the health database.
Conflict of interest statement
All (co-) authors declare that they have no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
