

A practical approach to detection and treatment of depression in Parkinson disease and dementia
- PMID: 28409063
- PMCID: PMC5386841
- DOI: 10.1212/CPJ.0000000000000351
A practical approach to detection and treatment of depression in Parkinson disease and dementia
Erratum in
-
Erratum: A practical approach to detection and treatment of depression in Parkinson disease and dementia.Neurol Clin Pract. 2018 Aug;8(4):278. doi: 10.1212/CPJ.0000000000000478. Neurol Clin Pract. 2018. PMID: 30140576 Free PMC article.
Abstract
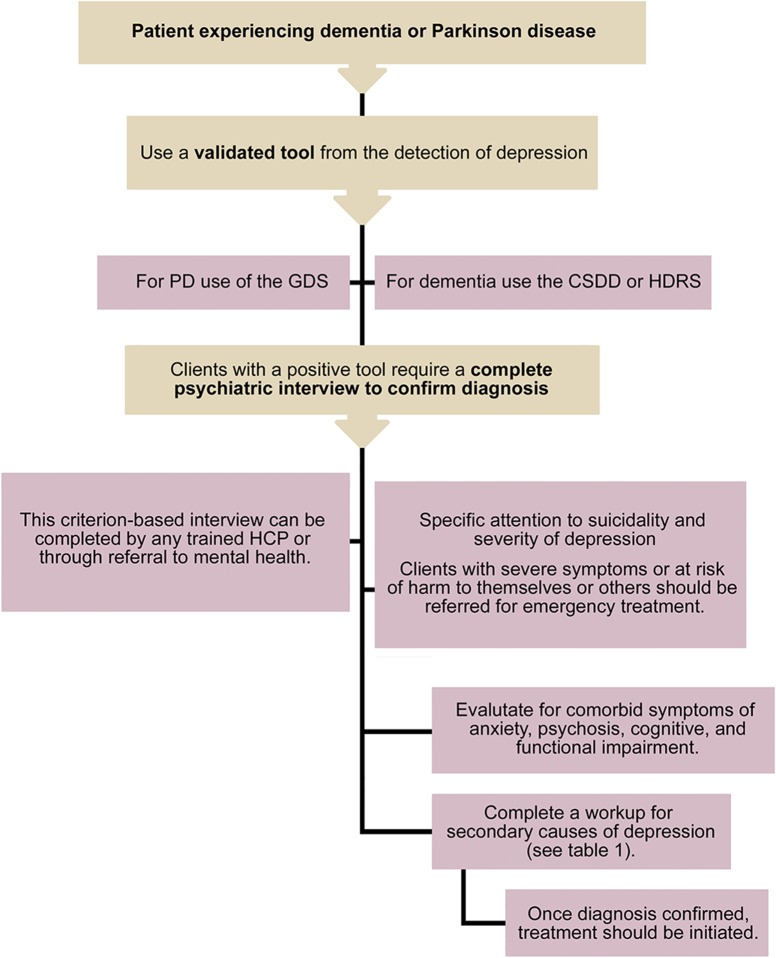
Purpose of review: To review the available evidence for the detection and management of depression in Parkinson disease (PD) and dementia.
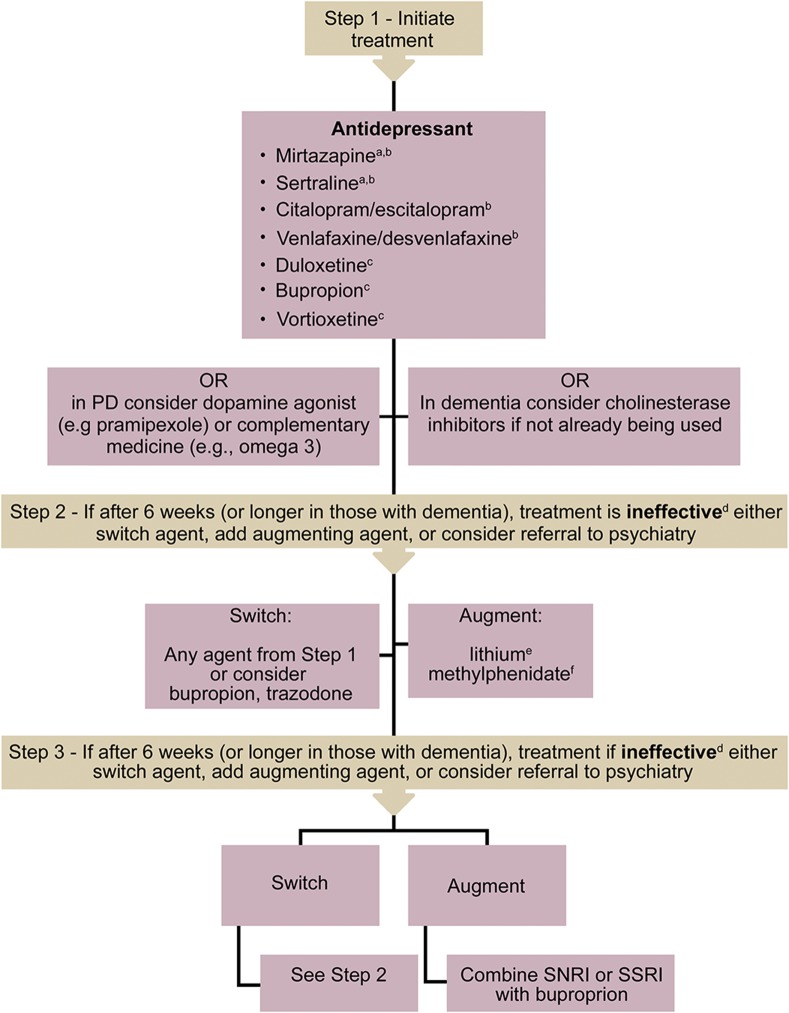
Recent findings: Depression is a common comorbidity in those with PD or dementia, and leads to increased morbidity. There are several available and accurate tools for the detection of depression in PD (e.g., Geriatric Depression Scale) and dementia (e.g., Cornell Scale for Depression in Dementia). Treatment of depression depends on patient preference, severity of depression, comorbidities, and available resources. Despite variable evidence, the use of nonpharmacologic strategies to manage depression is suggested. Pharmacologic management is guided by modest evidence in PD and dementia, but also informed by the management of late-life depression (LLD).
Summary: There is evidence to guide the diagnosis and management of depression in PD or dementia. However, more research is required in this field to better inform clinical decision-making.
Figures
Comment in
-
Neurology and mental health.Neurol Clin Pract. 2017 Apr;7(2):96-97. doi: 10.1212/CPJ.0000000000000345. Neurol Clin Pract. 2017. PMID: 29185550 Free PMC article. No abstract available.
References
-
- Djamshidian A, Friedman JH. Anxiety and depression in Parkinson's disease. Curr Treat Options Neurol 2014;16:285. - PubMed
-
- Ismail Z, Malick A, Smith EE, Schweizer T, Fischer C. Depression versus dementia: is this construct still relevant? Neurodegener Dis Manag 2014;4:119–126. - PubMed
-
- Knapskog AB, Barca ML, Engedal K. A comparison of the validity of the Cornell Scale and the MADRS in detecting depression among memory clinic patients. Dement Geriatr Cogn Disord 2011;32:287–294. - PubMed
-
- Pachana NA, Egan SJ, Laidlaw K, et al. Clinical issues in the treatment of anxiety and depression in older adults with Parkinson's disease. Mov Disord 2013;28:1930–1934. - PubMed
-
- Rocha FL, Murad MG, Stumpf BP, Hara C, Fuzikawa C. Antidepressants for depression in Parkinson's disease: systematic review and meta-analysis. J Psychopharmacol 2013;27:417–423. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials