

doi: 10.1016/j.eats.2016.09.036.
eCollection 2017 Feb.
Arthroscopic Technique for Stabilization of Chronic Acromioclavicular Joint Instability With Coracoclavicular and Acromioclavicular Ligament Reconstruction Using a Gracilis Tendon Graft
Affiliations
- PMID: 28409097
- PMCID: PMC5382553
- DOI: 10.1016/j.eats.2016.09.036
Item in Clipboard
Arthroscopic Technique for Stabilization of Chronic Acromioclavicular Joint Instability With Coracoclavicular and Acromioclavicular Ligament Reconstruction Using a Gracilis Tendon Graft
Arthrosc Tech.
.
Abstract
We present an arthroscopic technique for stabilization of chronic acromioclavicular (AC) joint instability using a transclavicular-transcoracoidal button technique, combined with a coracoclavicular and AC ligament reconstruction using the gracilis tendon. This arthroscopic technique achieves an anatomic reduction of the clavicle without further implant removal. It ensures vertical and horizontal stabilization of the AC joint. Using a horizontal drill hole through the clavicle and looping the gracilis tendon graft around the coracoid avoids weakening of the coracoid with the risk of fracture.
Figures

Four portals are required: standard posterior (A), anteromedial (B), anterolateral (C), and supracoracoidal (D), in addition to an incision 2 cm medial to the acromioclavicular joint.
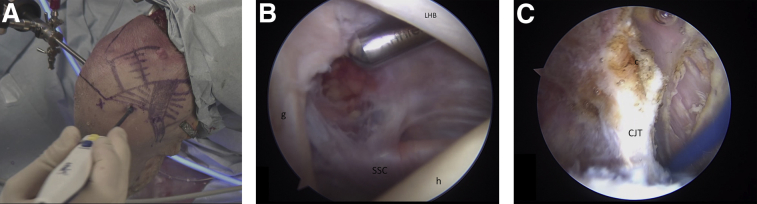
(A) Right shoulder, beach chair position—outside view. The arthroscope is in the dorsal standard portal (marked as A in Fig 1), the radiofrequency device is inserted through the anteromedial portal (marked as B in Fig 1). (B) The rotator interval is opened with a shaver to expose the anterior extra-articular space and to find the posterior surface of the coracoid. (C) With the help of a radiofrequency device, the coracoid is exposed posteriorly, laterally, and medially. The next step is to open the clavipectoral fascia. The conjoint tendons are exposed and the coracoid insertion of the CA ligament is detached. (c, coracoid; CJT, conjoint tendons; g, glenoid; h, humeral head; LHB, long head biceps tendon; SSC, M. subscapularis tendon.)

(A) Outside view. The camera is in the anterolateral viewing portal (marked as C in Fig 1). The radiofrequency device is inserted in the anteromedial portal (marked as B in Fig 1). (B) The undersurface of the coracoid and the CJ tendons are visualized. (CJ, conjoint tendons; SSC, upper border of the subscapularis tendon; X, undersurface of the coracoid.)

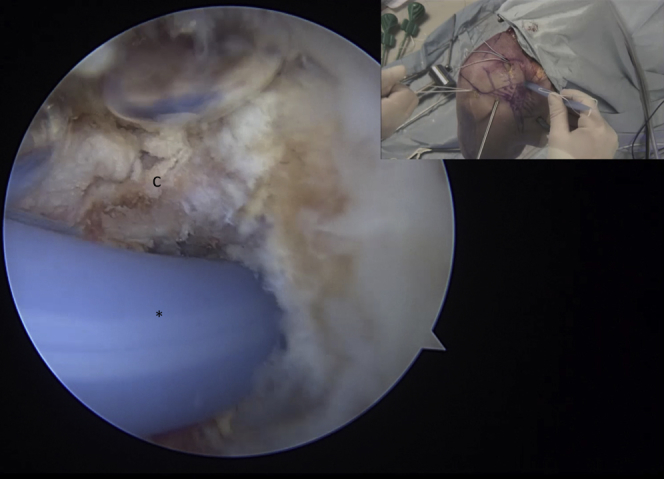
(A) To enhance the view, the deltoid muscle is retracted with a switching stick from the anterolateral portal (marked as C in Fig 1). The arthroscope is in the anteromedial portal (marked as B in Fig 1), and the radiofrequency device is in the supracoracoidal portal (marked as D in Fig 1). (B) The medial part of the coracoid is now visualized from extra-articular. The superior third of the insertion of the m. pectoralis minor is detached. ∗Created space for further passage of the graft around the coracoid. (c, coracoid; pm, pectoralis minor tendon.)

Arthroscopic and outside view. A transclavicular and transcoracoidal hole is drilled and a cortical button is placed in the posterior aspect of the coracoid knee. The second cortical button is placed 2 cm medial to the acromioclavicular joint in the middle of the anterior posterior dimension of the clavicle. The primary reduction is made by knot tying on top of the second cortical button. (c, coracoid; SSC, upper border of the m. subscapularis.)

A specific arthroscopic Dechamps is used for graft passage. It is inserted in the supracoracoidal portal (marked as D in Fig 1) around the medial aspect of the coracoid.
A flexible graft dilator is used to make a good gracilis graft passage. It is pulled from the medial supracoracoidal portal (marked as D in Fig 1) to the anterolateral portal (marked as C in Fig 1). ∗Flexible graft dilator. (c, coracoid.)

The looped end of the graft dilator is used to pull the prepared gracilis tendon around the coracoid from medial to lateral. The gracilis tendon is anterior to the cortical button. (c, coracoid; gr, gracilis tendon graft.)

Lateral to the previously placed cortical button, a K-wire is drilled through the clavicle in a sagittal direction from anterior to posterior. The K-wire is overdrilled with a 4.5-mm drill. ∗Cortical button. (cl, clavicle.)

(A) By using a nitinol wire, 2 FiberWires (Arthrex), which are used as shuttle sutures later, are pulled through the sagittal clavicular drill hole. One loop is placed anteriorly (x) and the other one posteriorly (y). (B) A KingFisher suture retriever (Arthrex) is inserted from anterior to the clavicle in an antero-inferior direction, and the lateral end of the gracilis tendon graft is retrieved. ∗Lateral end of the gracilis tendon graft. (C) Through the trapezius fascia, posterior to the clavicle the medial end of the gracilis tendon is retrieved. ∗Medial end of the gracilis tendon graft. (D) Both graft ends are retrieved. The medial end of the tendon graft (x) is posterior, and the lateral graft end (y) anterior, to the clavicle. ∗Gracilis tendon graft. (c, coracoid; cl, clavicle; kf, KingFisher posterior to the clavicle.)

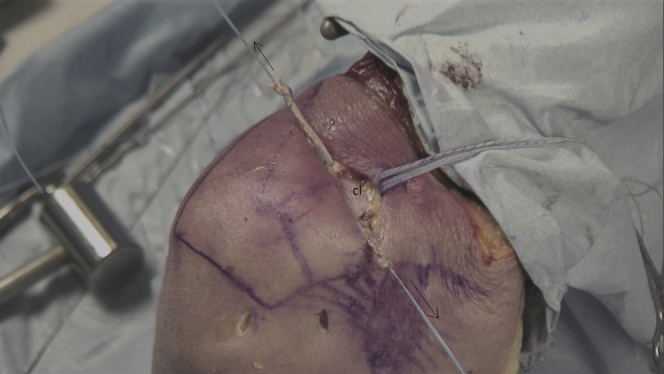
The graft is looped in a figure-of-8 around the coracoid, the medial part of the tendon is anterior to the lateral one. (c, coracoid; x, lateral end of graft; y, medial end of graft.)
With the earlier-placed shuttle sutures, the free ends of the gracilis tendon are now pulled against each other in the sagittal drill hole of the clavicle. (cl, clavicle.)

Under tension on both ends, a SwiveLock 4.75-mm biocomposite anchor (Arthrex) is inserted from anterior to posterior in the drill hole.
References
-
- Boström Windhamre H.A., von Heideken J.P., Une-Larsson V.E., Ekelund A.L. Surgical treatment of chronic acromioclavicular dislocations: A comparative study of Weaver-Dunn augmented with PDS-braid or hook plate. J Shoulder Elbow Surg. 2010;19:1040–1048. - PubMed
-
- Yoo J.C., Ahn J.H., Yoon J.R., Yang J.H. Clinical results of single-tunnel coracoclavicular ligament reconstruction using autogenous semitendinosus tendon. Am J Sports Med. 2010;38:950–957. - PubMed
-
- Scheibel M., Ifesanya A., Pauly S., Haas N.P. Arthroscopically assisted coracoclavicular ligament reconstruction for chronic acromioclavicular joint instability. Arch Orthop Trauma Surg. 2008;128:1327–1333. - PubMed
-
- Hosseini H., Friedmann S., Tröger M., Lobenhoffer P., Agneskirchner J.D. Arthroscopic reconstruction of chronic AC joint dislocations by transposition of the coracoacromial ligament augmented by the Tight Rope device: A technical note. Knee Surg Sports Traumatol Arthrosc. 2009;17:92–97. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
