Impact of Comorbidities Among Medicaid Enrollees With Chronic Obstructive Pulmonary Disease, United States, 2009
- PMID: 28409741
- PMCID: PMC5392445
- DOI: 10.5888/pcd14.160333
Impact of Comorbidities Among Medicaid Enrollees With Chronic Obstructive Pulmonary Disease, United States, 2009
Abstract
Introduction: Multimorbidity, the presence of 2 or more chronic conditions, frequently affects people with chronic obstructive pulmonary disease (COPD). Many have high-cost, highly complex conditions that have a substantial impact on state Medicaid programs. We quantified the cost of Medicaid-insured patients with COPD co-diagnosed with other chronic disorders.
Methods: We used nationally representative Medicaid claims data to analyze the impact of comorbidities (other chronic conditions) on the disease burden, emergency department (ED) use, hospitalizations, and total health care costs among 291,978 adult COPD patients. We measured the prevalence of common conditions and their influence on COPD-related and non-COPD-related resource use by using the Elixhauser Comorbidity Index. Elixhauser comorbidity counts were clustered from 0 to 7 or more. We performed multivariable logistic regression to determine the odds of ED visits by Elixhauser scores adjusting for age, sex, race/ethnicity, and residence.
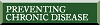
Results: Acute care, hospital bed days, and total Medicaid-reimbursed costs increased as the number of comorbidities increased. ED visits unrelated to COPD were more common than visits for COPD, especially in patients self-identified as black or African American (designated black). Hypertension, diabetes, affective disorders, hyperlipidemia, and asthma were the most prevalent comorbid disorders. Substance abuse, congestive heart failure, and asthma were commonly associated with ED visits for COPD. Female sex was associated with COPD-related and non-COPD-related ED visits.
Conclusion: Comorbidities markedly increased health services use among people with COPD insured with Medicaid, although ED visits in this study were predominantly unrelated to COPD. Achieving excellence in clinical practice with optimal clinical and economic outcomes requires a whole-person approach to the patient and a multidisciplinary health care team.
Figures
References
-
- Kochanek KD, Xu J, Murphy SL, Miniño AM, Kung HC. Deaths: final data for 2009. Natl Vital Stat Rep 2011;60(3):1–116. - PubMed
-
- Ni H, Xu J. COPD-related mortality by sex and race among adults aged 25 and over: United States, 2000–2014. Hyatsville (MD): National Center for Health Statistics, 2016.
-
- Lurie N, Popkin M, Dysken M, Moscovice I, Finch M. Accuracy of diagnoses of schizophrenia in Medicaid claims. Hosp Community Psychiatry 1992;43(1):69–71. - PubMed
Publication types
MeSH terms
Grants and funding
- R01 HL089897/HL/NHLBI NIH HHS/United States
- U54 MD007588/MD/NIMHD NIH HHS/United States
- KL2 TR000455/TR/NCATS NIH HHS/United States
- U01 HL089897/HL/NHLBI NIH HHS/United States
- R01 HL089856/HL/NHLBI NIH HHS/United States
- U01 HL089856/HL/NHLBI NIH HHS/United States
- UL1 TR000454/TR/NCATS NIH HHS/United States
- R25 MD007589/MD/NIMHD NIH HHS/United States
- P20 MD006881/MD/NIMHD NIH HHS/United States
- K18 HS022444/HS/AHRQ HHS/United States
- G12 MD007602/MD/NIMHD NIH HHS/United States
- U54 MD008149/MD/NIMHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical