

Three Hypothetical Inflammation Pathobiology Phenotypes and Pediatric Sepsis-Induced Multiple Organ Failure Outcome
- PMID: 28410274
- PMCID: PMC5457354
- DOI: 10.1097/PCC.0000000000001122
Three Hypothetical Inflammation Pathobiology Phenotypes and Pediatric Sepsis-Induced Multiple Organ Failure Outcome
Abstract
Objectives: We hypothesize that three inflammation pathobiology phenotypes are associated with increased inflammation, proclivity to develop features of macrophage activation syndrome, and multiple organ failure-related death in pediatric severe sepsis.
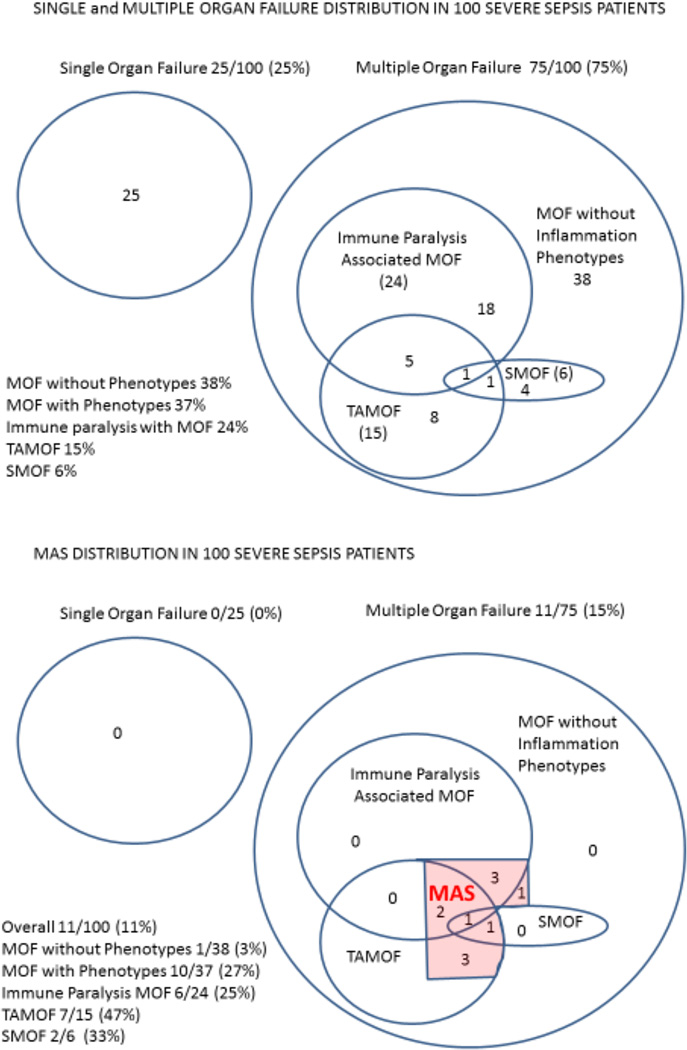
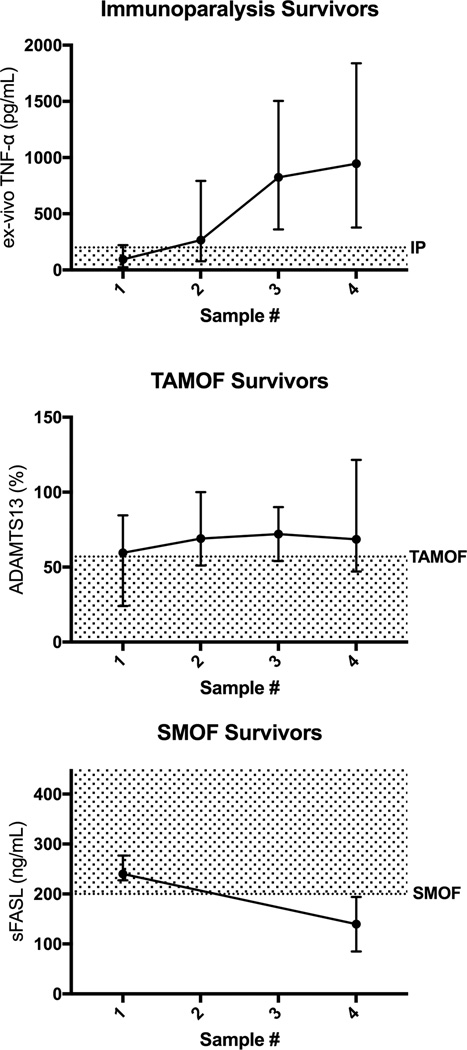
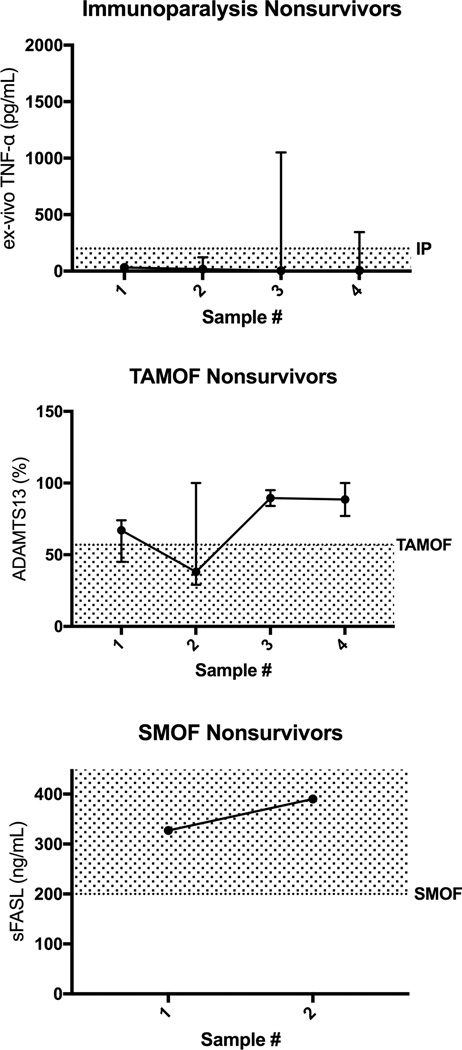
Design: Prospective cohort study comparing children with severe sepsis and any of three phenotypes: 1) immunoparalysis-associated multiple organ failure (whole blood ex vivo tumor necrosis factor response to endotoxin < 200 pg/mL), 2) thrombocytopenia-associated multiple organ failure (new onset thrombocytopenia with acute kidney injury and a disintegrin and metalloproteinase with a thrombospondin type 1 motif, member 13 activity < 57%), and/or 3) sequential multiple organ failure with hepatobiliary dysfunction (respiratory distress followed by liver dysfunction with soluble Fas ligand > 200 pg/mL), to those without any of these phenotypes.
Setting: Tertiary children's hospital PICU.
Patients: One hundred consecutive severe sepsis admissions.
Interventions: Clinical data were recorded daily, and blood was collected twice weekly.
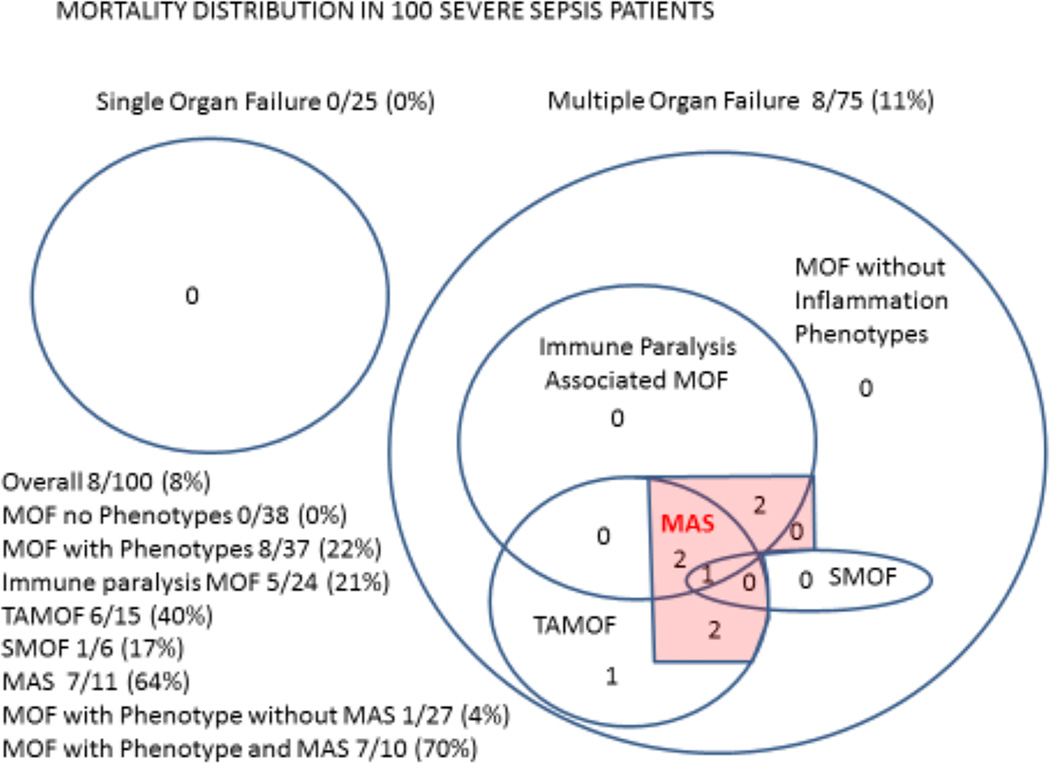
Measurements and main results: Multiple organ failure developed in 75 cases and eight died. Multiple organ failure cases with any of the three inflammation phenotypes (n = 37) had higher inflammation (C-reactive protein, p = 0.009 and ferritin, p < 0.001) than multiple organ failure cases without any of these phenotypes (n = 38) or cases with only single organ failure (n = 25). Development of features of macrophage activation syndrome and death were more common among multiple organ failure cases with any of the phenotypes (macrophage activation syndrome: 10/37, 27%; death: 8/37, 22%) compared to multiple organ failure cases without any phenotype (macrophage activation syndrome: 1/38, 3%; p = 0.003 and death: 0/38, 0%; p = 0.002).
Conclusions: Our approach to phenotype categorization remains hypothetical, and the phenotypes identified need to be confirmed in multicenter studies of pediatric multiple organ dysfunction syndrome.
Conflict of interest statement
Figures
Comment in
-
Sepsis Subclasses: Be Careful of What You Wish for.Pediatr Crit Care Med. 2017 Jun;18(6):591-592. doi: 10.1097/PCC.0000000000001132. Pediatr Crit Care Med. 2017. PMID: 28574905 Free PMC article. No abstract available.
Similar articles
-
A Multicenter Network Assessment of Three Inflammation Phenotypes in Pediatric Sepsis-Induced Multiple Organ Failure.Pediatr Crit Care Med. 2019 Dec;20(12):1137-1146. doi: 10.1097/PCC.0000000000002105. Pediatr Crit Care Med. 2019. PMID: 31568246 Free PMC article.
-
Hypofibrinogenemia Is Associated With Poor Outcome and Secondary Hemophagocytic Lymphohistiocytosis/Macrophage Activation Syndrome in Pediatric Severe Sepsis.Pediatr Crit Care Med. 2018 May;19(5):397-405. doi: 10.1097/PCC.0000000000001507. Pediatr Crit Care Med. 2018. PMID: 29470247 Free PMC article.
-
New or Progressive Multiple Organ Dysfunction Syndrome in Pediatric Severe Sepsis: A Sepsis Phenotype With Higher Morbidity and Mortality.Pediatr Crit Care Med. 2017 Jan;18(1):8-16. doi: 10.1097/PCC.0000000000000978. Pediatr Crit Care Med. 2017. PMID: 28060151 Free PMC article.
-
Pathophysiology of Pediatric Multiple Organ Dysfunction Syndrome.Pediatr Crit Care Med. 2017 Mar;18(3_suppl Suppl 1):S32-S45. doi: 10.1097/PCC.0000000000001052. Pediatr Crit Care Med. 2017. PMID: 28248832 Free PMC article. Review.
-
Rationale for Adjunctive Therapies for Pediatric Sepsis Induced Multiple Organ Failure.Pediatr Clin North Am. 2017 Oct;64(5):1071-1088. doi: 10.1016/j.pcl.2017.06.007. Epub 2017 Aug 18. Pediatr Clin North Am. 2017. PMID: 28941536 Free PMC article. Review.
Cited by
-
A Multicenter Network Assessment of Three Inflammation Phenotypes in Pediatric Sepsis-Induced Multiple Organ Failure.Pediatr Crit Care Med. 2019 Dec;20(12):1137-1146. doi: 10.1097/PCC.0000000000002105. Pediatr Crit Care Med. 2019. PMID: 31568246 Free PMC article.
-
Ferritin: An Inflammatory Player Keeping Iron at the Core of Pathogen-Host Interactions.Microorganisms. 2020 Apr 18;8(4):589. doi: 10.3390/microorganisms8040589. Microorganisms. 2020. PMID: 32325688 Free PMC article. Review.
-
Clinical Sepsis Phenotypes in Critically Ill Patients.Microorganisms. 2023 Aug 27;11(9):2165. doi: 10.3390/microorganisms11092165. Microorganisms. 2023. PMID: 37764009 Free PMC article. Review.
-
Adults with septic shock and extreme hyperferritinemia exhibit pathogenic immune variation.Genes Immun. 2019 Jul;20(6):520-526. doi: 10.1038/s41435-018-0030-3. Epub 2018 Jul 6. Genes Immun. 2019. PMID: 29977033 Free PMC article. Clinical Trial.
-
Inhibition of XBP1 Alleviates LPS-Induced Cardiomyocytes Injury by Upregulating XIAP through Suppressing the NF-κB Signaling Pathway.Inflammation. 2021 Jun;44(3):974-984. doi: 10.1007/s10753-020-01392-w. Epub 2021 Jan 16. Inflammation. 2021. PMID: 33453047
References
-
- Watson RS, Carcillo JA, Linde-Zwirble WT, et al. The epidemiology of severe sepsis in children in the United States. Am J Respir Crit Care Med. 2003;167(5):695–701. - PubMed
-
- Felmet KA, Hall MW, Clark RS, et al. Prolonged lymphopenia, lymphoid depletion, and hypoprolactinemia in children with nosocomial sepsis and multiple organ failure. J Immunol. 2005;174(6):3765–3772. - PubMed
-
- Volk HD, Reinke P, Döcke WD. Clinical aspects: from systemic inflammation to 'immunoparalysis'. Chem Immunol. 2000;74:162–177. - PubMed
MeSH terms
Grants and funding
- R01 GM108618/GM/NIGMS NIH HHS/United States
- U10 HD063108/HD/NICHD NIH HHS/United States
- U10 HD050012/HD/NICHD NIH HHS/United States
- UG1 HD049983/HD/NICHD NIH HHS/United States
- U10 HD049981/HD/NICHD NIH HHS/United States
- U10 HD050096/HD/NICHD NIH HHS/United States
- U10 HD049983/HD/NICHD NIH HHS/United States
- U10 HD063106/HD/NICHD NIH HHS/United States
- UG1 HD063108/HD/NICHD NIH HHS/United States
- R01 GM113838/GM/NIGMS NIH HHS/United States
- U10 HD063114/HD/NICHD NIH HHS/United States
- U01 HD049934/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
