

Worldwide comparison of survival from childhood leukaemia for 1995-2009, by subtype, age, and sex (CONCORD-2): a population-based study of individual data for 89 828 children from 198 registries in 53 countries
- PMID: 28411119
- PMCID: PMC5418564
- DOI: 10.1016/S2352-3026(17)30052-2
Worldwide comparison of survival from childhood leukaemia for 1995-2009, by subtype, age, and sex (CONCORD-2): a population-based study of individual data for 89 828 children from 198 registries in 53 countries
Erratum in
-
Correction to Lancet Haematol 2017; 4: e202-17.Lancet Haematol. 2017 May;4(5):e201. doi: 10.1016/S2352-3026(17)30067-4. Lancet Haematol. 2017. PMID: 28460816 Free PMC article. No abstract available.
Abstract
Background: Global inequalities in access to health care are reflected in differences in cancer survival. The CONCORD programme was designed to assess worldwide differences and trends in population-based cancer survival. In this population-based study, we aimed to estimate survival inequalities globally for several subtypes of childhood leukaemia.
Methods: Cancer registries participating in CONCORD were asked to submit tumour registrations for all children aged 0-14 years who were diagnosed with leukaemia between Jan 1, 1995, and Dec 31, 2009, and followed up until Dec 31, 2009. Haematological malignancies were defined by morphology codes in the International Classification of Diseases for Oncology, third revision. We excluded data from registries from which the data were judged to be less reliable, or included only lymphomas, and data from countries in which data for fewer than ten children were available for analysis. We also excluded records because of a missing date of birth, diagnosis, or last known vital status. We estimated 5-year net survival (ie, the probability of surviving at least 5 years after diagnosis, after controlling for deaths from other causes [background mortality]) for children by calendar period of diagnosis (1995-99, 2000-04, and 2005-09), sex, and age at diagnosis (<1, 1-4, 5-9, and 10-14 years, inclusive) using appropriate life tables. We estimated age-standardised net survival for international comparison of survival trends for precursor-cell acute lymphoblastic leukaemia (ALL) and acute myeloid leukaemia (AML).
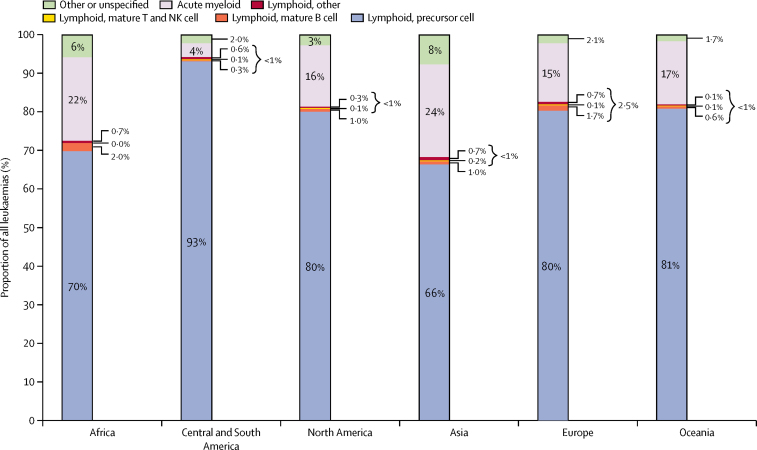
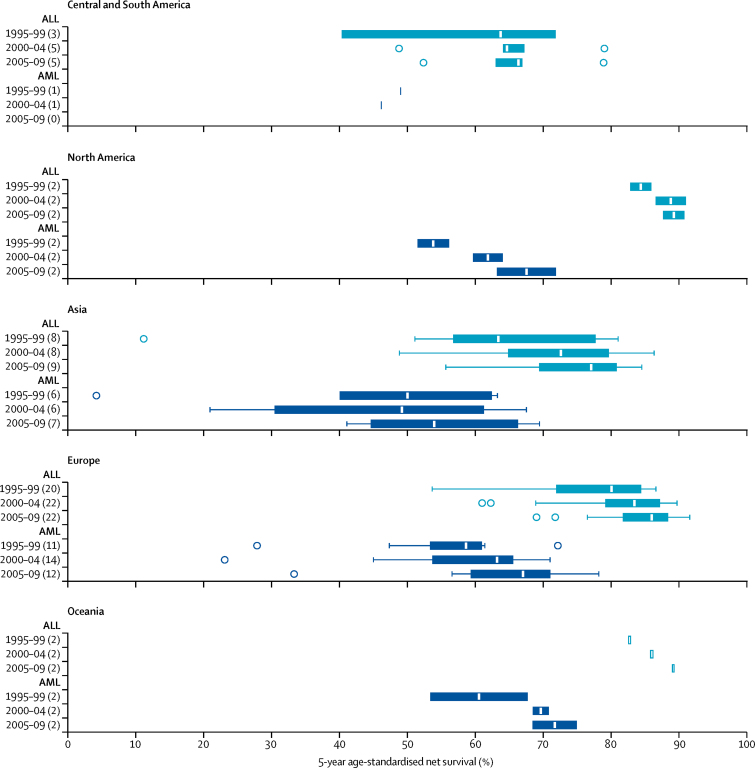
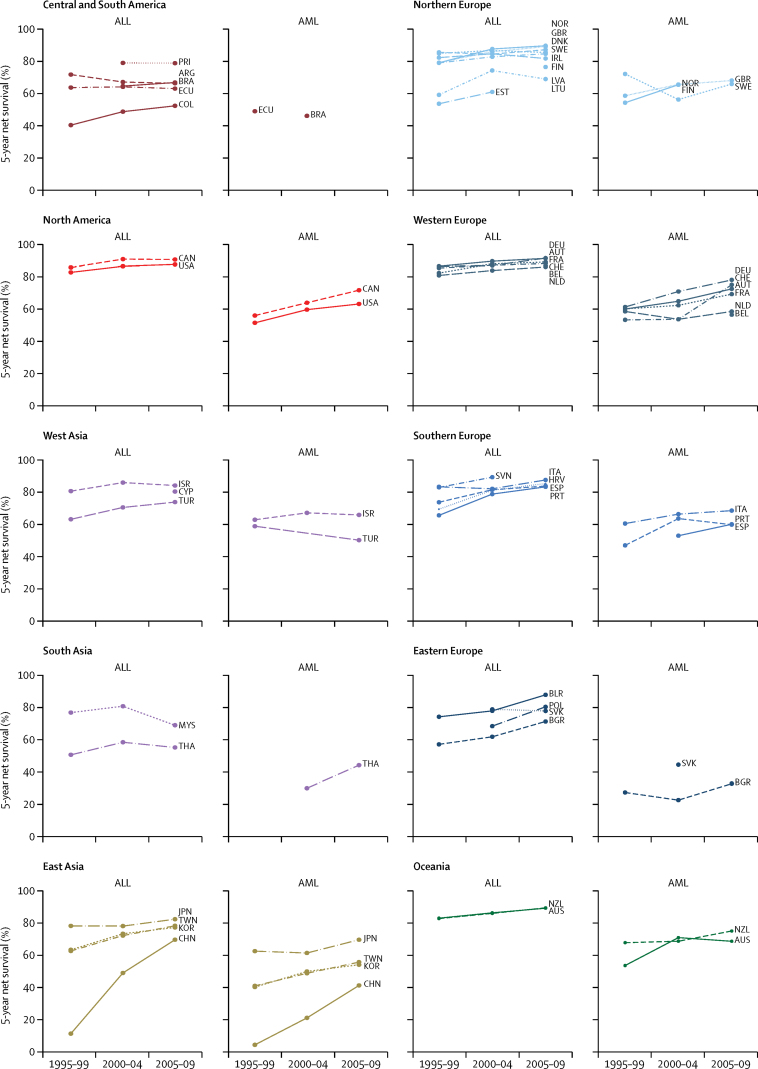
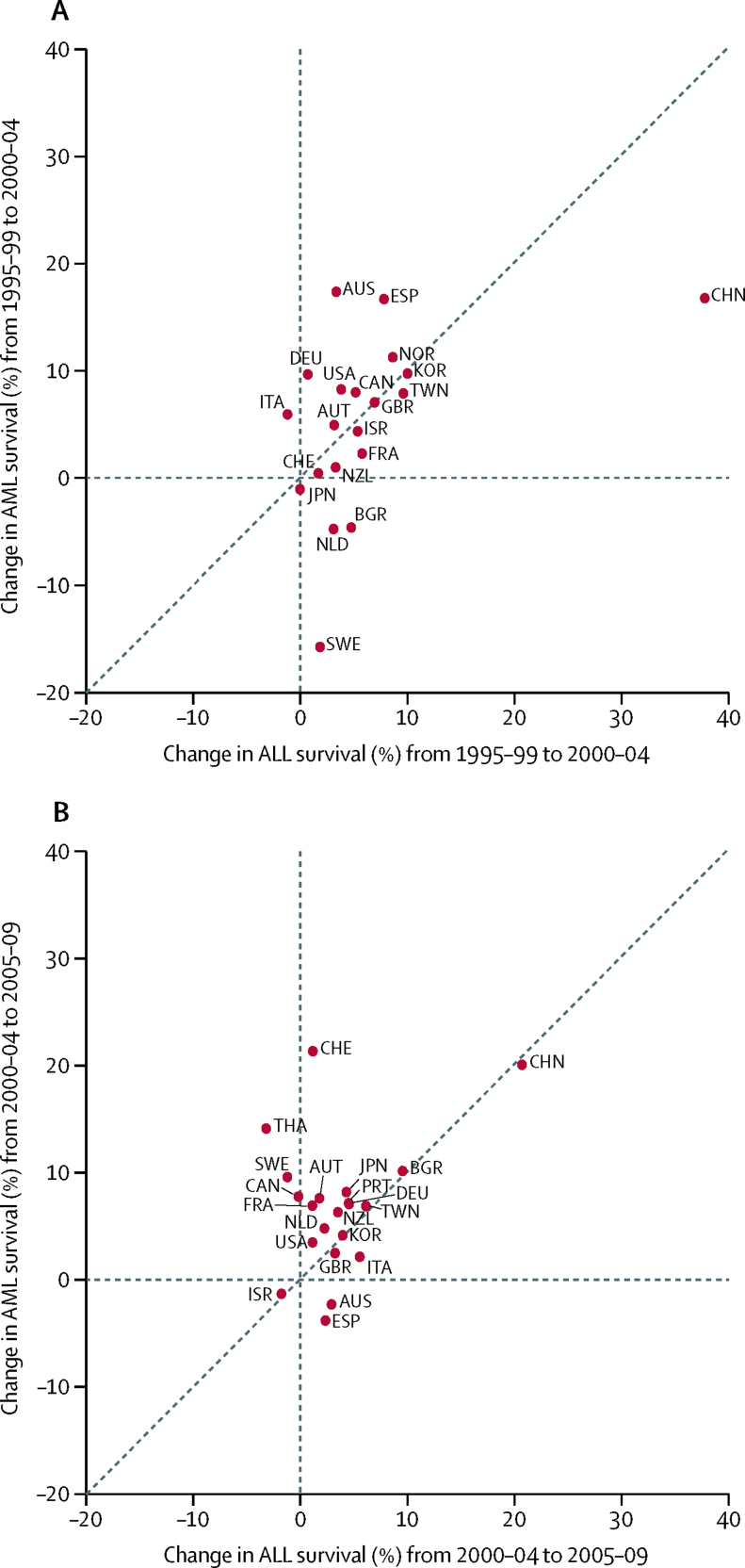
Findings: We analysed data from 89 828 children from 198 registries in 53 countries. During 1995-99, 5-year age-standardised net survival for all lymphoid leukaemias combined ranged from 10·6% (95% CI 3·1-18·2) in the Chinese registries to 86·8% (81·6-92·0) in Austria. International differences in 5-year survival for childhood leukaemia were still large as recently as 2005-09, when age-standardised survival for lymphoid leukaemias ranged from 52·4% (95% CI 42·8-61·9) in Cali, Colombia, to 91·6% (89·5-93·6) in the German registries, and for AML ranged from 33·3% (18·9-47·7) in Bulgaria to 78·2% (72·0-84·3) in German registries. Survival from precursor-cell ALL was very close to that of all lymphoid leukaemias combined, with similar variation. In most countries, survival from AML improved more than survival from ALL between 2000-04 and 2005-09. Survival for each type of leukaemia varied markedly with age: survival was highest for children aged 1-4 and 5-9 years, and lowest for infants (younger than 1 year). There was no systematic difference in survival between boys and girls.
Interpretation: Global inequalities in survival from childhood leukaemia have narrowed with time but remain very wide for both ALL and AML. These results provide useful information for health policy makers on the effectiveness of health-care systems and for cancer policy makers to reduce inequalities in childhood cancer survival.
Funding: Canadian Partnership Against Cancer, Cancer Focus Northern Ireland, Cancer Institute New South Wales, Cancer Research UK, US Centers for Disease Control and Prevention, Swiss Re, Swiss Cancer Research foundation, Swiss Cancer League, and the University of Kentucky.
Copyright © 2017 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Global improvements in childhood leukaemia survival.Lancet Haematol. 2017 May;4(5):e192. doi: 10.1016/S2352-3026(17)30061-3. Lancet Haematol. 2017. PMID: 28460812 No abstract available.
-
Do big numbers assure high-quality of data?Lancet Haematol. 2017 Jul;4(7):e309. doi: 10.1016/S2352-3026(17)30107-2. Lancet Haematol. 2017. PMID: 28668190 No abstract available.
References
-
- Ferlay J, Soerjomataram I, Dikshit R. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136:e359–e386. - PubMed
-
- Coleman MP, Quaresma M, Berrino F. Cancer survival in five continents: a worldwide population-based study (CONCORD) Lancet Oncol. 2008;9:730–756. - PubMed
-
- Magrath I, Steliarova-Foucher E, Epelman S. Paediatric cancer in low-income and middle-income countries. Lancet Oncol. 2013;14:e104–e116. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
