

Long-Term Follow-up of the PADI Trial: Percutaneous Transluminal Angioplasty Versus Drug-Eluting Stents for Infrapopliteal Lesions in Critical Limb Ischemia
- PMID: 28411244
- PMCID: PMC5533004
- DOI: 10.1161/JAHA.116.004877
Long-Term Follow-up of the PADI Trial: Percutaneous Transluminal Angioplasty Versus Drug-Eluting Stents for Infrapopliteal Lesions in Critical Limb Ischemia
Abstract
Background: Clinical outcomes reported after treatment of infrapopliteal lesions with drug-eluting stents (DESs) have been more favorable compared with percutaneous transluminal angioplasty with a bailout bare metal stent (PTA-BMS) through midterm follow-up in patients with critical limb ischemia. In the present study, long-term results of treatment of infrapopliteal lesions with DESs are presented.
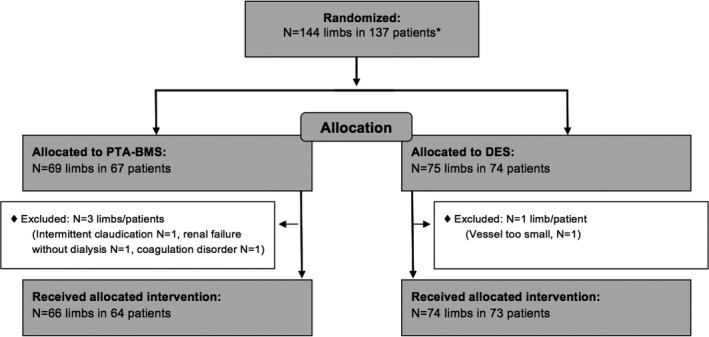
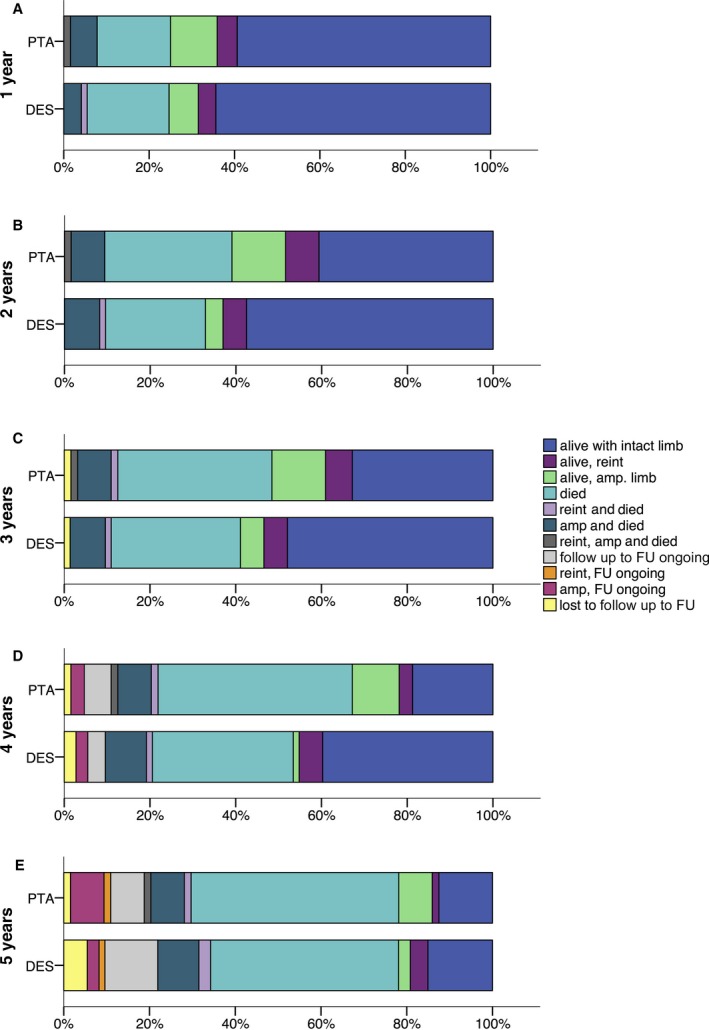
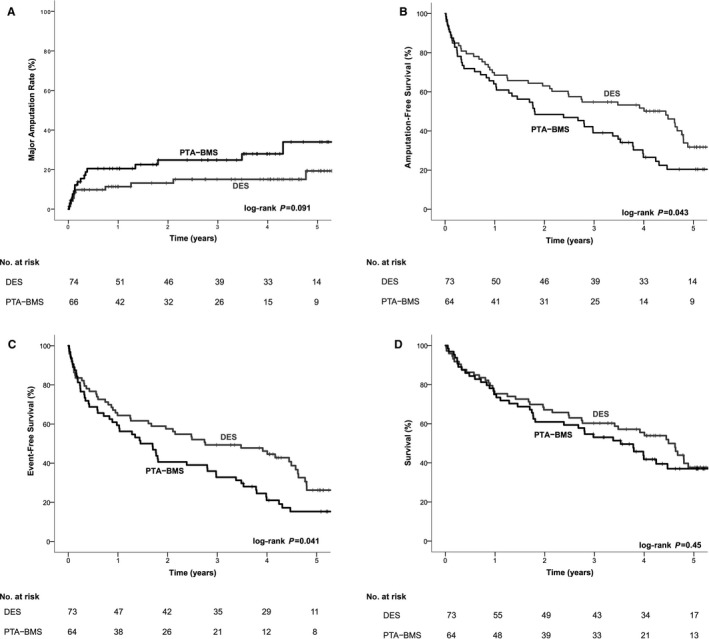
Methods and results: Adults with critical limb ischemia (Rutherford category ≥4) and infrapopliteal lesions were randomized to receive PTA-BMS or DESs with paclitaxel. Long-term follow-up consisted of annual assessments up to 5 years after treatment or until a clinical end point was reached. Clinical end points were major amputation (above ankle level), infrapopliteal surgical or endovascular reintervention, and death. Preserved primary patency (≤50% restenosis) of treated lesions was an additional morphological end point, assessed by duplex sonography. In total, 74 limbs (73 patients) were treated with DESs and 66 limbs (64 patients) were treated with PTA-BMS. The estimated 5-year major amputation rate was lower in the DES arm (19.3% versus 34.0% for PTA-BMS; P=0.091). The 5-year rates of amputation- and event-free survival (survival free from major amputation or reintervention) were significantly higher in the DES arm compared with PTA-BMS (31.8% versus 20.4%, P=0.043; and 26.2% versus 15.3%, P=0.041, respectively). Survival rates were comparable. The limited available morphological results showed higher preserved patency rates after DESs than after PTA-BMS at 1, 3, and 4 years of follow-up.
Conclusions: Both clinical and morphological long-term results after treatment of infrapopliteal lesions in patients with critical limb ischemia are improved with DES compared with PTA-BMS.
Clinical trial registration: URL: http://www.clinicaltrials.gov. Unique identifier: NCT00471289.
Keywords: critical limb ischemia; drug‐eluting stent; endovascular treatment; peripheral artery disease.
© 2017 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
References
-
- Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FG. Inter‐society consensus for the management of peripheral arterial disease (TASC II). J Vasc Surg. 2007;45(suppl S):S5–S67. - PubMed
-
- Hirsch AT, Haskal ZJ, Hertzer NR, Bakal CW, Creager MA, Halperin JL, Hiratzka LF, Murphy WR, Olin JW, Puschett JB, Rosenfield KA, Sacks D, Stanley JC, Taylor LM Jr, White CJ, White J, White RA, Antman EM, Smith SC Jr, Adams CD, Anderson JL, Faxon DP, Fuster V, Gibbons RJ, Hunt SA, Jacobs AK, Nishimura R, Ornato JP, Page RL, Riegel B. ACC/AHA guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): a collaborative report from the American Associations for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (writing committee to develop guidelines for the management of patients with peripheral arterial disease)–summary of recommendations. J Vasc Interv Radiol. 2006;17:1383–1397; quiz 1398. - PubMed
-
- Adam DJ, Beard JD, Cleveland T, Bell J, Bradbury AW, Forbes JF, Fowkes FG, Gillepsie I, Ruckley CV, Raab G, Storkey H. Bypass versus angioplasty in severe ischaemia of the leg (BASIL): multicentre, randomised controlled trial. Lancet. 2005;366:1925–1934. - PubMed
-
- Nehler MR, Coll JR, Hiatt WR, Regensteiner JG, Schnickel GT, Klenke WA, Strecker PK, Anderson MW, Jones DN, Whitehill TA, Moskowitz S, Krupski WC. Functional outcome in a contemporary series of major lower extremity amputations. J Vasc Surg. 2003;38:7–14. - PubMed
-
- van Overhagen H, Spiliopoulos S, Tsetis D. Below‐the‐knee interventions. Cardiovasc Intervent Radiol. 2013;36:302–311. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
