

Noninvasive FFR Derived From Coronary CT Angiography: Management and Outcomes in the PROMISE Trial
- PMID: 28412436
- PMCID: PMC5632098
- DOI: 10.1016/j.jcmg.2016.11.024
Noninvasive FFR Derived From Coronary CT Angiography: Management and Outcomes in the PROMISE Trial
Abstract
Objectives: The purpose of this study was to determine whether noninvasive fractional flow reserve derived from computed tomography (FFRCT) predicts coronary revascularization and outcomes and whether its addition improves efficiency of referral to invasive coronary angiography (ICA) after coronary computed tomography angiography (CTA).
Background: FFRCT may improve the efficiency of an anatomic CTA strategy for stable chest pain.
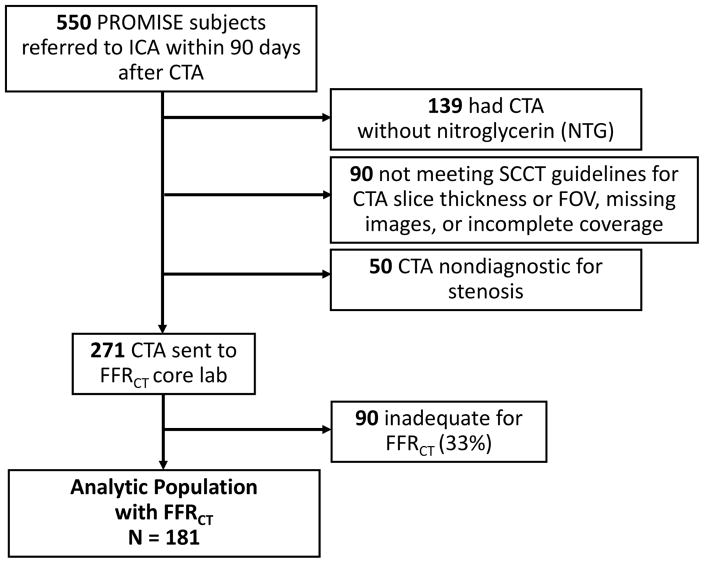
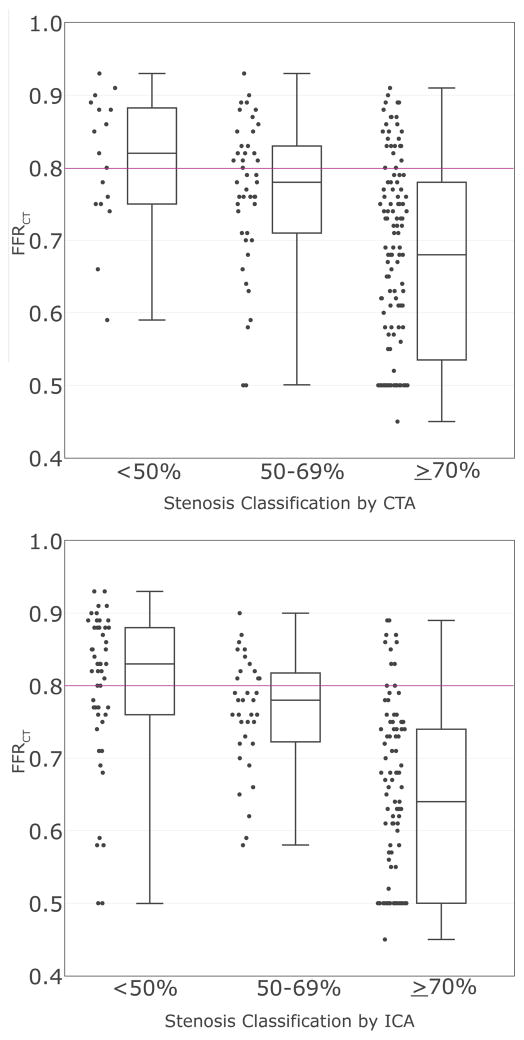
Methods: This observational cohort study included patients with stable chest pain in the PROMISE (PROspective Multicenter Imaging Study for Evaluation of Chest Pain) trial referred to ICA within 90 days after CTA. FFRCT was measured at a blinded core laboratory, and FFRCT results were unavailable to caregivers. We determined the agreement of FFRCT (positive if ≤0.80) with stenosis on CTA and ICA (positive if ≥50% left main or ≥70% other coronary artery), and predictive value for a composite of coronary revascularization or major adverse cardiac events (death, myocardial infarction, or unstable angina). We retrospectively assessed whether adding FFRCT ≤0.80 as a gatekeeper could improve efficiency of referral to ICA, defined as decreased rate of ICA without ≥50% stenosis and increased ICA leading to revascularization.
Results: FFRCT was calculated in 67% (181 of 271) of eligible patients (mean age 62 years; 36% women). FFRCT was discordant with stenosis in 31% (57 of 181) for CTA and 29% (52 of 181) for ICA. Most patients undergoing coronary revascularization had an FFRCT of ≤0.80 (91%; 80 of 88). An FFRCT of ≤0.80 was a significantly better predictor for revascularization or major adverse cardiac events than severe CTA stenosis (HR: 4.3 [95% confidence interval [CI]: 2.4 to 8.9] vs. 2.9 [95% CI: 1.8 to 5.1]; p = 0.033). Reserving ICA for patients with an FFRCT of ≤0.80 could decrease ICA without ≥50% stenosis by 44%, and increase the proportion of ICA leading to revascularization by 24%.
Conclusions: In this hypothesis-generating study of patients with stable chest pain referred to ICA from CTA, an FFRCT of ≤0.80 was a better predictor of revascularization or major adverse cardiac events than severe stenosis on CTA. Adding FFRCT may improve efficiency of referral to ICA from CTA alone.
Keywords: computational fluid dynamics; coronary angiography; coronary artery disease; coronary computed tomography angiography; fractional flow reserve.
Copyright © 2017 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Coronary Artery Disease Testing: Past, Present, and Future.JACC Cardiovasc Imaging. 2017 Nov;10(11):1359-1360. doi: 10.1016/j.jcmg.2016.11.023. Epub 2017 Apr 12. JACC Cardiovasc Imaging. 2017. PMID: 28412417 No abstract available.
Similar articles
-
Selective FFRCT testing in suspected stable angina in clinical practice - initial experiences.Int J Cardiovasc Imaging. 2024 Oct;40(10):2213-2220. doi: 10.1007/s10554-024-03214-8. Epub 2024 Sep 11. Int J Cardiovasc Imaging. 2024. PMID: 39259436 Free PMC article.
-
Fractional flow reserve derived from coronary computed tomography angiography reclassification rate using value distal to lesion compared to lowest value.J Cardiovasc Comput Tomogr. 2017 Nov;11(6):462-467. doi: 10.1016/j.jcct.2017.09.009. Epub 2017 Sep 21. J Cardiovasc Comput Tomogr. 2017. PMID: 28986147
-
1-Year Impact on Medical Practice and Clinical Outcomes of FFRCT: The ADVANCE Registry.JACC Cardiovasc Imaging. 2020 Jan;13(1 Pt 1):97-105. doi: 10.1016/j.jcmg.2019.03.003. Epub 2019 Mar 17. JACC Cardiovasc Imaging. 2020. PMID: 31005540
-
Can Computed Fractional Flow Reserve Coronary CT Angiography (FFRCT) Offer an Accurate Noninvasive Comparison to Invasive Coronary Angiography (ICA)? "The Noninvasive CATH." A Comprehensive Review.Curr Probl Cardiol. 2021 Mar;46(3):100642. doi: 10.1016/j.cpcardiol.2020.100642. Epub 2020 Jun 3. Curr Probl Cardiol. 2021. PMID: 32624193 Review.
-
Interpreting results of coronary computed tomography angiography-derived fractional flow reserve in clinical practice.J Cardiovasc Comput Tomogr. 2017 Sep-Oct;11(5):383-388. doi: 10.1016/j.jcct.2017.06.002. Epub 2017 Jun 23. J Cardiovasc Comput Tomogr. 2017. PMID: 28666784 Review.
Cited by
-
Is it the Time to Move Towards Coronary Computed Tomography Angiography-Derived Fractional Flow Reserve Guided Percutaneous Coronary Intervention? The Pros and Cons.Curr Cardiol Rev. 2023;19(4):e190123212887. doi: 10.2174/1573403X19666230119115228. Curr Cardiol Rev. 2023. PMID: 36658709 Free PMC article. Review.
-
Diagnostic accuracy of CCTA-derived versus angiography-derived quantitative flow ratio (CAREER) study: a prospective study protocol.BMJ Open. 2022 Jun 23;12(6):e055481. doi: 10.1136/bmjopen-2021-055481. BMJ Open. 2022. PMID: 35738652 Free PMC article.
-
Low Wall Shear Stress Is Associated with Saphenous Vein Graft Stenosis in Patients with Coronary Artery Bypass Grafting.J Cardiovasc Transl Res. 2021 Aug;14(4):770-781. doi: 10.1007/s12265-020-09982-7. Epub 2020 Apr 2. J Cardiovasc Transl Res. 2021. PMID: 32240496 Free PMC article.
-
Predictive value of coronary artery computed tomography-derived fractional flow reserve for cardiovascular events in patients with coronary artery disease.Herz. 2024 Aug;49(4):296-301. doi: 10.1007/s00059-023-05220-3. Epub 2023 Nov 3. Herz. 2024. PMID: 37923966 English.
-
CAD-RADS - a new clinical decision support tool for coronary computed tomography angiography.Eur Radiol. 2018 Apr;28(4):1365-1372. doi: 10.1007/s00330-017-5105-4. Epub 2017 Nov 7. Eur Radiol. 2018. PMID: 29116390 Free PMC article. Review.
References
-
- Budoff MJ, Dowe D, Jollis JG, et al. Diagnostic performance of 64-multidetector row coronary computed tomographic angiography for evaluation of coronary artery stenosis in individuals without known coronary artery disease: results from the prospective multicenter ACCURACY (Assessment by Coronary Computed Tomographic Angiography of Individuals Undergoing Invasive Coronary Angiography) trial. J Am Coll Cardiol. 2008;52:1724–32. - PubMed
-
- Meijboom WB, Meijs MF, Schuijf JD, et al. Diagnostic accuracy of 64-slice computed tomography coronary angiography: a prospective, multicenter, multivendor study. J Am Coll Cardiol. 2008;52:2135–44. - PubMed
-
- Tonino PA, Fearon WF, De Bruyne B, et al. Angiographic versus functional severity of coronary artery stenoses in the FAME study fractional flow reserve versus angiography in multivessel evaluation. J Am Coll Cardiol. 2010;55:2816–21. - PubMed
-
- Budoff MJ, Nakazato R, Mancini GB, et al. CT Angiography for the Prediction of Hemodynamic Significance in Intermediate and Severe Lesions: Head-to-Head Comparison With Quantitative Coronary Angiography Using Fractional Flow Reserve as the Reference Standard. J Am Coll Cardiol Img. 2016;9:559–564. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
