

Early application of low-dose glucocorticoid improves acute respiratory distress syndrome: A meta-analysis of randomized controlled trials
- PMID: 28413460
- PMCID: PMC5377286
- DOI: 10.3892/etm.2017.4154
Early application of low-dose glucocorticoid improves acute respiratory distress syndrome: A meta-analysis of randomized controlled trials
Abstract
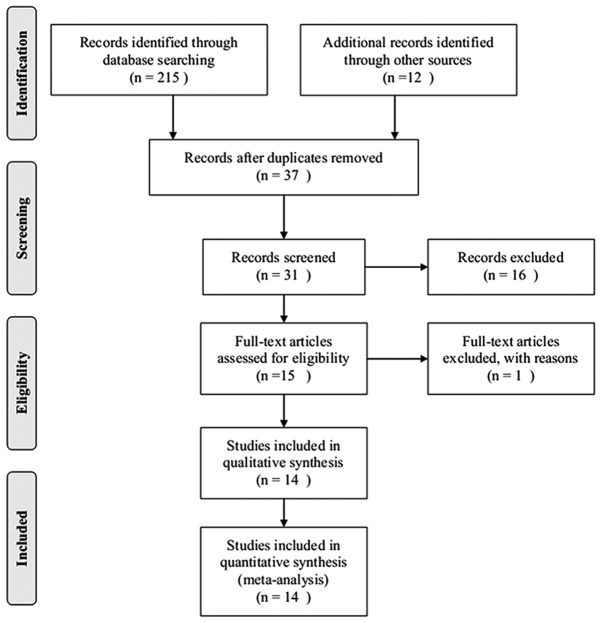
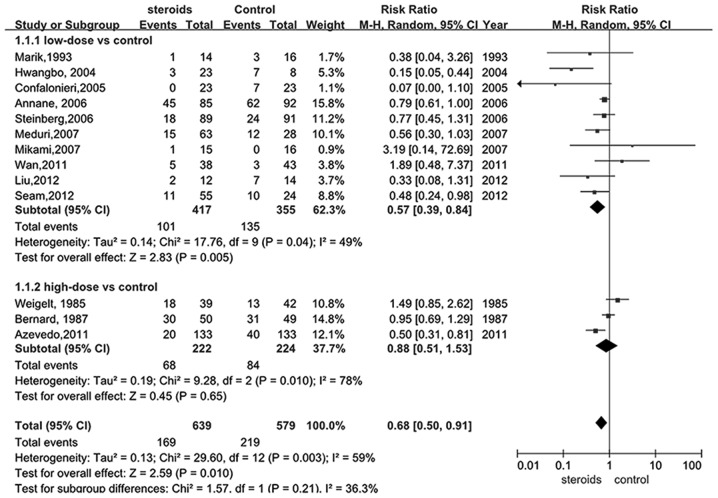
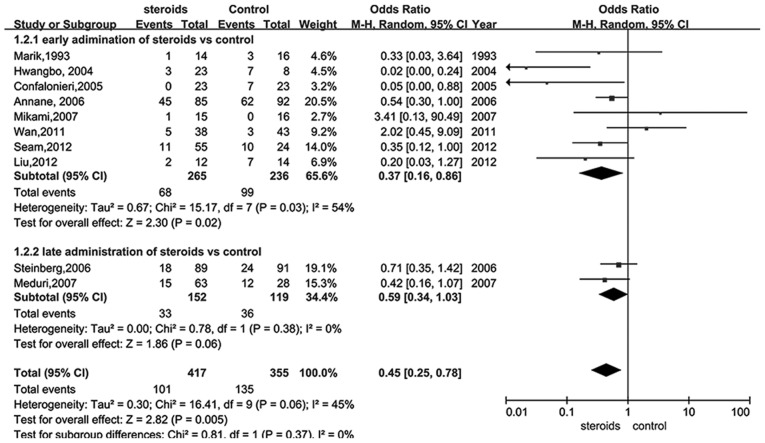
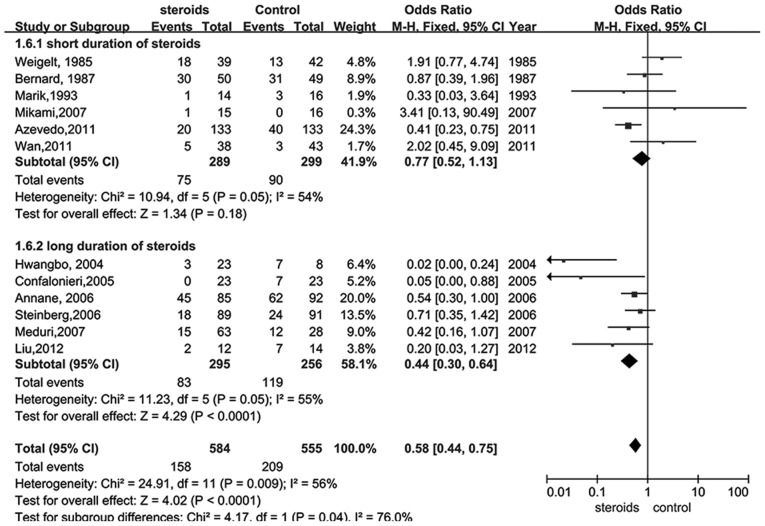
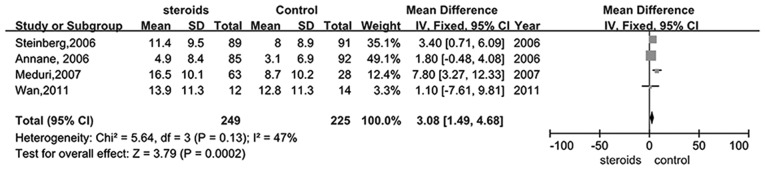
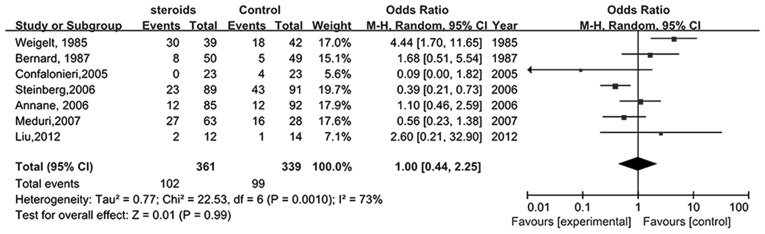
Previous clinical trials have investigated the effect of glucocorticoid therapy in acute respiratory distress syndrome (ARDS), with controversial results, particularly with regard to the early administration of low dose glucocorticoid. The present meta-analysis aimed to assess whether the application of glucocorticoid was able to reduce mortality in patients with ARDS. A literature search was performed using online databases, including MEDLINE, Embase, Cochrane and CNKI regardless of whether the studies were published in English or Chinese. Following assessment via inclusion and exclusion criteria, two reviewers screened controlled randomized trials which investigated glucocorticoid therapy in ARDS patients and independently extracted data. The quality of all of the included trials was evaluated based on blinding, randomization and other methods. A total of 14 studies with 1,441 patients met the inclusion criteria. The results of the meta-analysis demonstrated that glucocorticoid significantly reduced the overall mortality of patients with ARDS [relative ratio (RR), 0.68; 95% confidence interval (CI), 0.50-0.91; P<0.05], particularly with a low-dose of glucocorticoid (RR, 0.57; 95% CI, 0.39-0.84; P<0.05) at the early phase of ARDS (RR, 0.37; 95% CI, 0.16-0.86; P<0.05), and a longer duration of steroids (RR, 0.44; 95% CI, 0.30-0.64; P<0.05). Administration of steroids also significantly increased the number of days that patients remained alive and were off mechanical ventilation (RR, 3.08; 95% CI, 1.49-4.68; P<0.05) without significantly increasing the novel infection rate (RR, 1.00; 95% CI, 0.44-2.25; P<0.05). Due to inconsistencies and other limitations, the quality of the studies used for the meta-analysis of the effect of glucocorticoid on mortality was low. In conclusion, early use of low dose glucocorticoid may effectively reduce mortality in patients with ARDS. However, this conclusion may be affected by the limited quality of the studies included in the present meta-analysis.
Keywords: acute respiratory distress syndrome; effect; glucocorticoid; meta-analysis; mortality.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous