

American Society for Enhanced Recovery (ASER) and Perioperative Quality Initiative (POQI) joint consensus statement on optimal analgesia within an enhanced recovery pathway for colorectal surgery: part 1-from the preoperative period to PACU
- PMID: 28413629
- PMCID: PMC5390366
- DOI: 10.1186/s13741-017-0064-5
American Society for Enhanced Recovery (ASER) and Perioperative Quality Initiative (POQI) joint consensus statement on optimal analgesia within an enhanced recovery pathway for colorectal surgery: part 1-from the preoperative period to PACU
Abstract
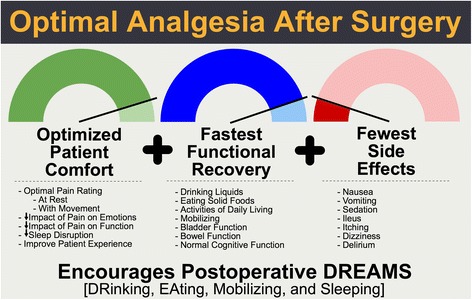
Background: Within an enhanced recovery pathway (ERP), the approach to treating pain should be multifaceted and the goal should be to deliver "optimal analgesia," which we define in this paper as a technique that optimizes patient comfort and facilitates functional recovery with the fewest medication side effects.
Methods: With input from a multi-disciplinary, international group of clinicians, and through a structured review of the literature and use of a modified Delphi method, we achieved consensus surrounding the topic of optimal analgesia in the perioperative period for colorectal surgery patients.
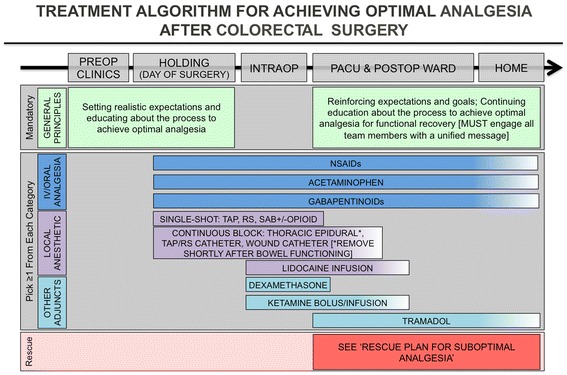
Discussion: As a part of the first Perioperative Quality Improvement (POQI) workgroup meeting, we sought to develop a consensus document describing a comprehensive, yet rational and practical, approach for developing an evidence-based plan for achieving optimal analgesia, specifically for a colorectal surgery ERP. The goal was two-fold: (a) that application of this process would lead to improved patient outcomes and (b) that investigation of the questions raised would identify knowledge gaps to aid the direction for research into analgesia within ERPs in the years to come. This document details the evidence for a wide range of analgesic components, with particular focus from the preoperative period to the post-anesthesia care unit. The overall conclusion is that the combination of analgesic techniques employed in the perioperative period is not important as long as it is effective in delivering the goal of optimal analgesia as set forth in this document.
Keywords: Colorectal; Enhanced recovery pathway; Multimodal; Non-opioid adjuncts; Optimal analgesia; Outcomes; Pain management; Perioperative; Quality.
Figures
References
-
- Abdallah FW, Dwyer T, Chan VW, Niazi AU, Ogilvie-Harris DJ, Oldfield S, Patel R, Oh J, Brull R. IV and perineural dexmedetomidine similarly prolong the duration of analgesia after interscalene brachial plexus block: a randomized, three-arm, triple-masked, placebo-controlled trial. Anesthesiology. 2016;124:683–95. doi: 10.1097/ALN.0000000000000983. - DOI - PubMed
-
- Akkaya A, Yildiz I, Tekelioglu UY, Demirhan A, Bayir H, Ozlu T, Bilgi M, Kocoglu H. Dexamethasone added to levobupivacaine in ultrasound-guided tranversus abdominis plain block increased the duration of postoperative analgesia after caesarean section: a randomized, double blind, controlled trial. Eur Rev Med Pharmacol Sci. 2014;18:717–22. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
