

Anorectal functional outcome following laparoscopic low anterior resection for rectal cancer
- PMID: 28413679
- PMCID: PMC5374898
- DOI: 10.3892/mco.2017.1183
Anorectal functional outcome following laparoscopic low anterior resection for rectal cancer
Abstract
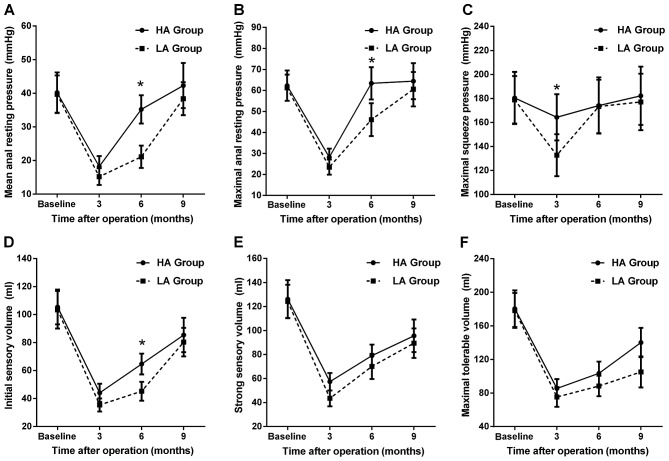
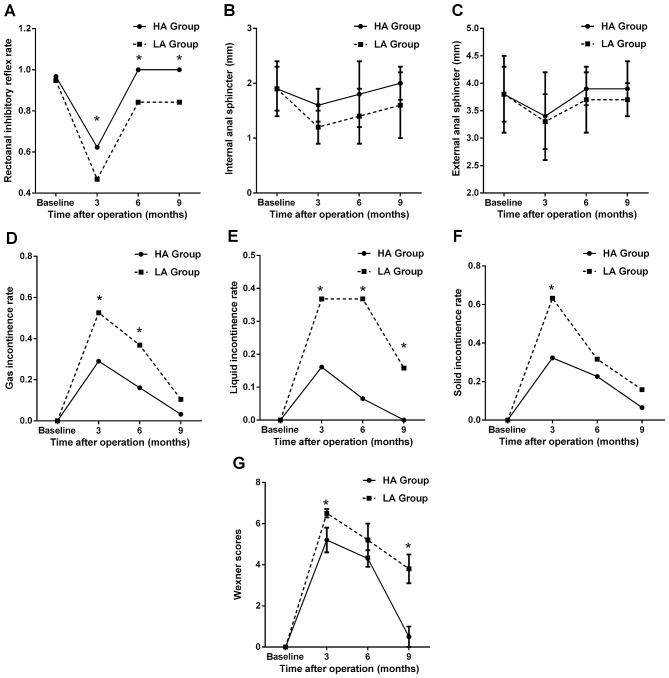
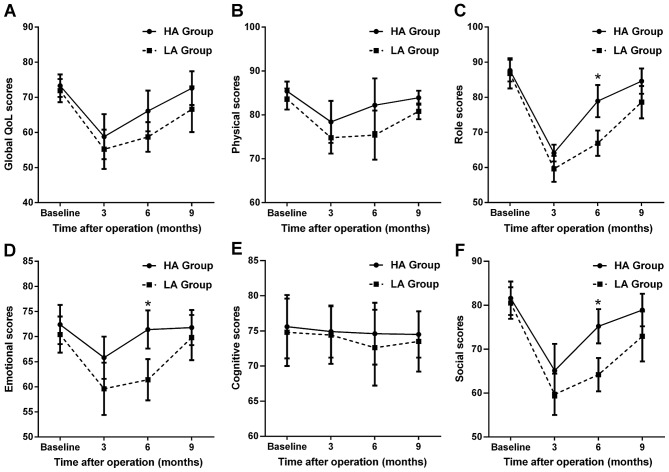
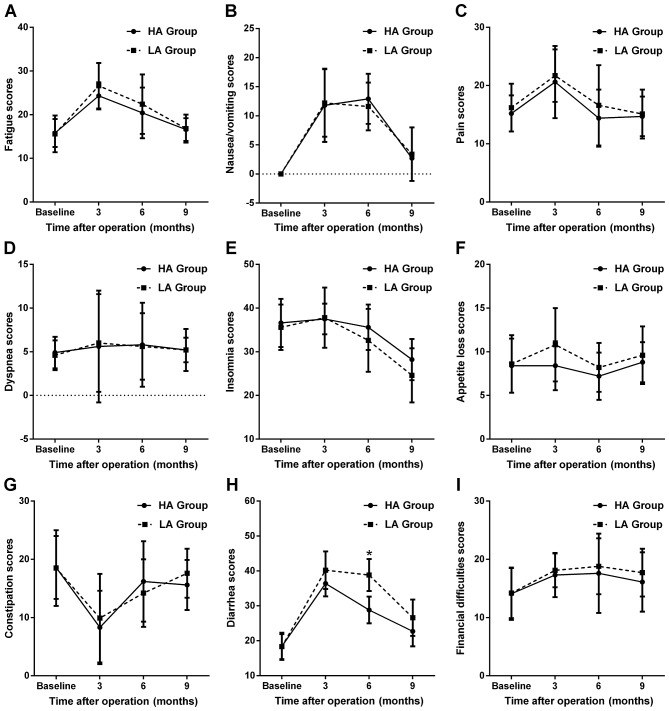
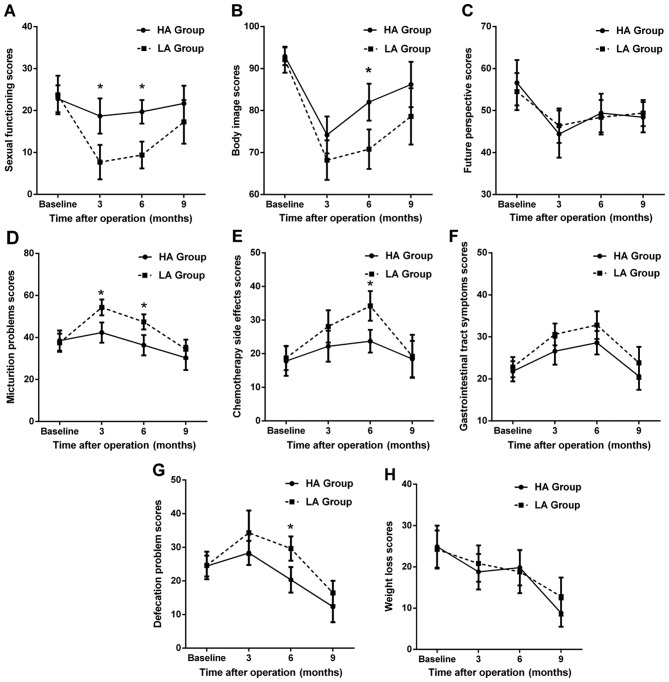
Low anterior resection (LAR) with total mesorectal excision has been considered a standard treatment for patients with rectal cancer. However, the functional outcome and life quality of laparoscopic LAR (LLAR) in Chinese patients remain unclear. A cohort of 51 Chinese patients (22 men and 29 women) who had undergone LLAR was included in this study. Anorectal manometry combined with the Wexner scores questionnaire were applied to assess functional outcome preoperatively (1 week) and postoperatively (at 3, 6 and 9 months). The validated Chinese versions of the European Organization for Research and Treatment of Cancer QLQ-C30 and QLQ-CR38 questionnaires were also used to assess the patients' quality of life at the indicated time points. The results demonstrated that the manometric parameters exhibited a temporary decrease at 3 months postoperatively, but a gradual increase at 6 and 9 months, while the Wexner scores exhibited an opposite trend. Furthermore, patients with high anastomoses had significantly higher manometric parameters, a lower frequency of incontinence and lower Wexner scores compared with those with low anastomoses at 9 months (all P<0.05). For the entire cohort, quality of life at 3 months postoperatively was worse compared with the preoperative level, but returned to normal by 9 months. Patients with high anastomoses exhibited significantly better role, emotional and social function, had a better body image and sexual function, fewer problems with defecation and lower frequency of diarrhea, as well as fewer chemotherapy-related side effects at 6 months postoperatively when compared with the low anastomosis group (all P<0.05). In conclusion, LLAR is generally acceptable for Chinese patients with rectal cancer, particularly for those with middle or high rectal cancer, in terms of functional outcome and quality of life.
Keywords: anorectal function; laparoscopic low anterior resection; manometry; rectal cancer.
Figures
Similar articles
-
Long-term effects of neoadjuvant chemoradiotherapy followed by sphincter-preserving resection on anal sphincter function in relation to quality of life among locally advanced rectal cancer patients: a cross-sectional analysis.Radiat Oncol. 2015 Aug 12;10:168. doi: 10.1186/s13014-015-0479-4. Radiat Oncol. 2015. PMID: 26264590 Free PMC article.
-
Usefulness of Anorectal Manometry for Diagnosing Continence Problems After a Low Anterior Resection.Ann Coloproctol. 2016 Jun;32(3):101-4. doi: 10.3393/ac.2016.32.3.101. Epub 2016 Jun 30. Ann Coloproctol. 2016. PMID: 27437391 Free PMC article.
-
A comparison of the long-term anorectal function between laparoscopic intersphincteric resection and low anterior resection for low rectal cancer.Surg Today. 2018 Oct;48(10):921-927. doi: 10.1007/s00595-018-1669-0. Epub 2018 May 11. Surg Today. 2018. PMID: 29752529
-
Functional outcome of low rectal resection evaluated by anorectal manometry.ANZ J Surg. 2018 Jun;88(6):E512-E516. doi: 10.1111/ans.14207. Epub 2017 Sep 18. ANZ J Surg. 2018. PMID: 28922706
-
What Are the Best Questionnaires To Capture Anorectal Function After Surgery in Rectal Cancer?Curr Colorectal Cancer Rep. 2015;11(1):37-43. doi: 10.1007/s11888-014-0217-6. Curr Colorectal Cancer Rep. 2015. PMID: 25663833 Free PMC article. Review.
Cited by
-
Assessing the role of anastomotic level in low anterior resection (LAR) surgery among rectal cancer patients in the development of LAR syndrome: a systematic review study.BMC Surg. 2023 Sep 1;23(1):263. doi: 10.1186/s12893-023-02166-5. BMC Surg. 2023. PMID: 37653424 Free PMC article.
-
Anthropometric Assessment After Proctocolectomy Due to Ulcerative Colitis.In Vivo. 2019 Jan-Feb;33(1):239-243. doi: 10.21873/invivo.11466. In Vivo. 2019. PMID: 30587630 Free PMC article.
-
Resting vector volume measured before ileostomy reversal may be a predictor of major fecal incontinence in patients with mid or low rectal cancer: a longitudinal cohort study using a prospective clinical database.Int J Colorectal Dis. 2019 Jun;34(6):1079-1086. doi: 10.1007/s00384-019-03293-3. Epub 2019 Apr 17. Int J Colorectal Dis. 2019. PMID: 30997602
-
When do defecation function and quality of life recover for patients with non-ostomy and ostomy surgery of rectal cancer?BMC Surg. 2020 Mar 30;20(1):57. doi: 10.1186/s12893-020-00719-6. BMC Surg. 2020. PMID: 32228547 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous