

Excess atherosclerosis in systemic lupus erythematosus,-A matter of renal involvement: Case control study of 281 SLE patients and 281 individually matched population controls
- PMID: 28414714
- PMCID: PMC5393555
- DOI: 10.1371/journal.pone.0174572
Excess atherosclerosis in systemic lupus erythematosus,-A matter of renal involvement: Case control study of 281 SLE patients and 281 individually matched population controls
Abstract
Background: Systemic lupus erythematosus (SLE), is a heterogeneous disease which predominantly affects young females (90%). SLE is associated with a shorter life expectancy than in the general population. Standardized mortality ratios (SMR) of 2.4 have been reported, which is comparable to diabetes. In modern societies cardiovascular disease (CVD) is the major cause of premature mortality. Accelerated atherosclerosis is generally assumed to be the underlying cause for SLE related CVD. However, previous studies diverge regarding whether atherosclerosis is more common in SLE than in controls. With this in mind and based on own clinical experience we hypothesized that accelerated atherosclerosis is not a general feature of SLE, but prevails in SLE subgroups.
Methods: 281 SLE patients and 281 individually age and sex matched population controls, were investigated clinically. Fasting blood samples and risk factor data were collected. All participants were subject to B-mode ultrasonography of the carotid arteries. Carotid plaque occurrence and mean intima media thickness (mIMT) were recorded. Two SLE subgroups previously described to be at high CVD risk; 1) patients with nephritis and 2) patients with anti-phospholipid antibodies (aPL), and one subgroup reported to be at comparatively lower CVD risk; patients positive for Sjögren´s syndrome antigens A/B (SSA/SSB) antibodies were analyzed separately in comparison with their respective matched controls.
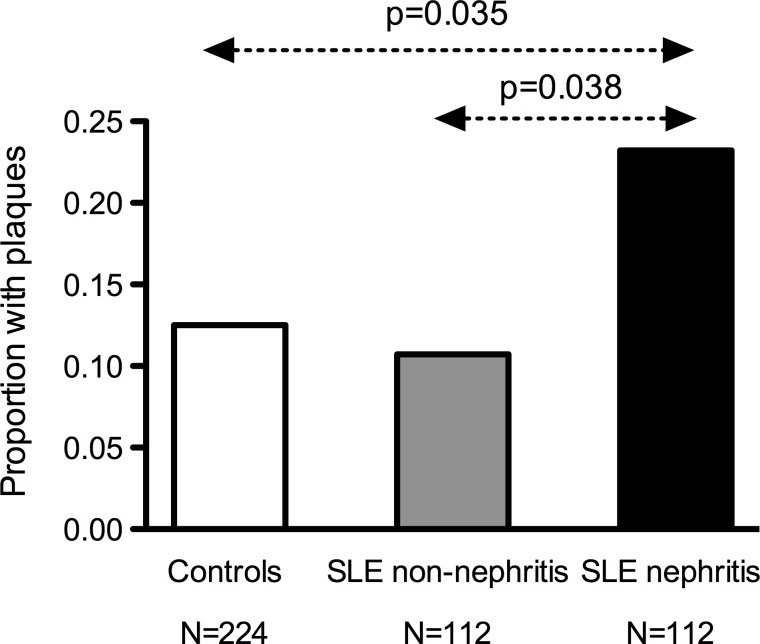
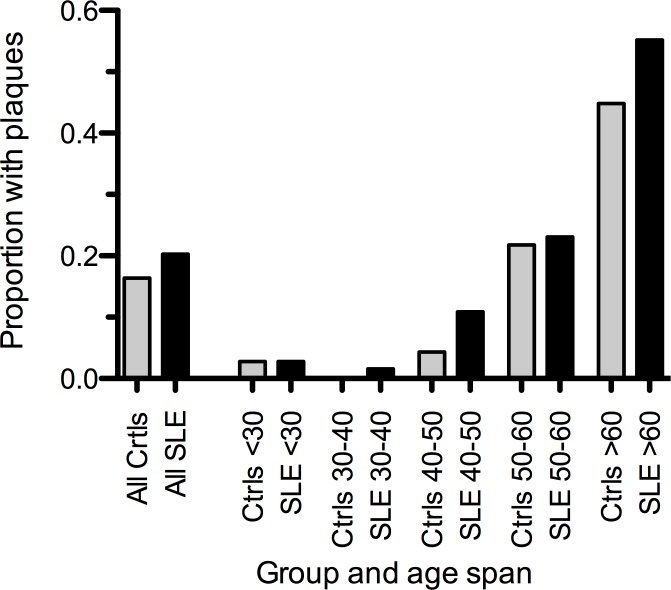
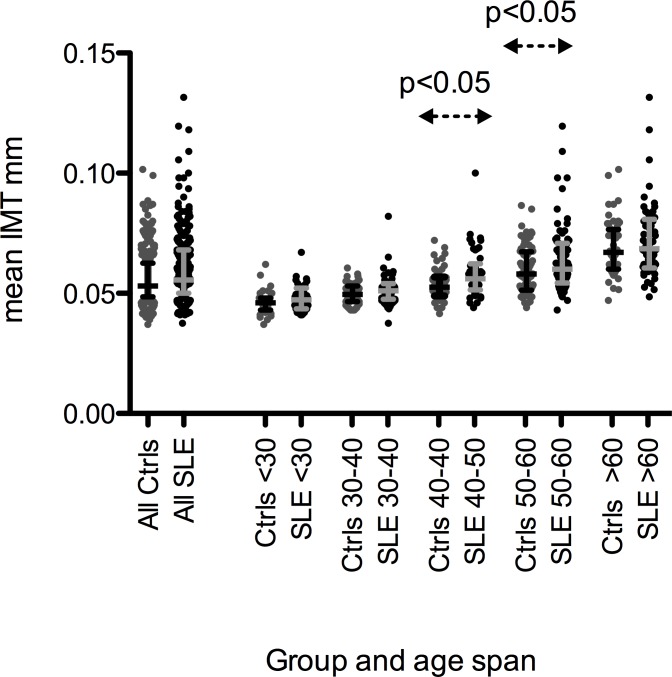
Results: Median age was 49 (IQR 36-59) years, 93% were females. Manifest CVD; ischemic heart, cerebro- and peripheral vascular disease, prevailed in patients (12% vs. 1%, p<0.0001). Overall plaque prevalence did not differ (20% vs. 16%), but patients had slightly higher mIMT than controls (0.56 vs. 0.53 mm, p<0.0033). After age adjustment plaques, but not mIMT, remained associated with previous CVD events. Therefore we focused further analyses on plaques, a more robust measure of atherosclerosis. Patients with nephritis (40%), but neither aPL (25%) nor SSA/SSB (40%) positive patients, had more plaques than their respective controls (23% vs. 11%, p = 0.008). Notably, patients with nephritis were younger than other SLE patients (45 vs.49 years, p = 0.02). To overcome the confounding effect of age we performed an age-matched nested case-control analysis, which demonstrated that patients with nephritis had twice as often plaques (23%) as both non-nephritis patients (11%, p = 0.038) and controls (12%, p = 0.035).
Conclusions: In SLE excess carotid plaques are essentially confined to the SLE subgroup with nephritis. This subgroup had plaques twice as often as age-matched non-nephritis SLE patients and population controls. Non-nephritis SLE patients, including the aPL positive subgroup, which has a high CVD risk, had similar prevalence of plaques as controls. To prevent later CVD events, this novel observation calls for risk factor screening and initiation of anti-atherosclerotic treatment selectively in SLE nephritis patients. Preferably at nephritis onset, which is often at a young age. In a general perspective this study demonstrates the importance to perform careful clinical subgroup analyses when investigating heterogeneous, hitherto not clearly defined, conditions like SLE.
Conflict of interest statement
Figures
Similar articles
-
[Risk factors of thickened intima-media and atherosclerotic plaque development in carotid arteries in patients with systemic lupus erythematosus].Ann Acad Med Stetin. 2008;54(2):22-32. Ann Acad Med Stetin. 2008. PMID: 19374227 Polish.
-
Similar progression of carotid intima-media thickness in 7-year surveillance of patients with mild SLE and controls, but this progression is still promoted by dyslipidaemia, lower HDL levels, hypertension, history of lupus nephritis and a higher prednisolone usage in patients.Lupus Sci Med. 2020 Jan 9;7(1):e000362. doi: 10.1136/lupus-2019-000362. eCollection 2020. Lupus Sci Med. 2020. PMID: 32095248 Free PMC article.
-
Lupus nephritis as an independent risk factor for carotid atherosclerosis in patients with systemic lupus erythematosus.Clin Rheumatol. 2025 May;44(5):1927-1937. doi: 10.1007/s10067-025-07413-z. Epub 2025 Mar 26. Clin Rheumatol. 2025. PMID: 40138152
-
SLE, atherosclerosis and cardiovascular disease.J Intern Med. 2005 Jun;257(6):485-95. doi: 10.1111/j.1365-2796.2005.01502.x. J Intern Med. 2005. PMID: 15910552 Review.
-
'Not only...but also': factors that contribute to accelerated atherosclerosis and premature coronary heart disease in systemic lupus erythematosus.Rheumatology (Oxford). 2005 Dec;44(12):1492-502. doi: 10.1093/rheumatology/kei142. Epub 2005 Oct 18. Rheumatology (Oxford). 2005. PMID: 16234277 Review.
Cited by
-
Endothelial Dysfunction in Systemic Lupus Erythematosus and Systemic Sclerosis: A Common Trigger for Different Microvascular Diseases.Front Med (Lausanne). 2022 Apr 8;9:849086. doi: 10.3389/fmed.2022.849086. eCollection 2022. Front Med (Lausanne). 2022. PMID: 35462989 Free PMC article. Review.
-
Choroidal thickness changes in systemic lupus erythematosus patients.Clin Ophthalmol. 2019 Aug 20;13:1567-1578. doi: 10.2147/OPTH.S219347. eCollection 2019. Clin Ophthalmol. 2019. PMID: 31933520 Free PMC article.
-
Protective Effects of Hydroxychloroquine against Accelerated Atherosclerosis in Systemic Lupus Erythematosus.Mediators Inflamm. 2018 Feb 18;2018:3424136. doi: 10.1155/2018/3424136. eCollection 2018. Mediators Inflamm. 2018. PMID: 29670462 Free PMC article. Review.
-
Elevation of serum proprotein convertase subtilisin/kexin type 9 (PCSK9) concentrations and its possible atherogenic role in patients with systemic lupus erythematosus.Ann Transl Med. 2018 Dec;6(23):452. doi: 10.21037/atm.2018.11.04. Ann Transl Med. 2018. PMID: 30603640 Free PMC article.
-
Impaired Microcirculation and Vascular Hemodynamics in Relation to Macrocirculation in Patients With Systemic Lupus Erythematosus.Front Med (Lausanne). 2021 Nov 1;8:722758. doi: 10.3389/fmed.2021.722758. eCollection 2021. Front Med (Lausanne). 2021. PMID: 34790671 Free PMC article.
References
-
- Bernatsky S, Boivin JF, Joseph L, Manzi S, Ginzler E, Gladman DD, et al. Mortality in systemic lupus erythematosus. Arthritis Rheum. 2006;54(8):2550–7. doi: 10.1002/art.21955 - DOI - PubMed
-
- Esdaile JM, Abrahamowicz M, Grodzicky T, Li Y, Panaritis C, du Berger R, et al. Traditional Framingham risk factors fail to fully account for accelerated atherosclerosis in systemic lupus erythematosus. Arthritis Rheum. 2001;44(10):2331–7. - PubMed
-
- Hak AE, Karlson EW, Feskanich D, Stampfer MJ, Costenbader KH. Systemic lupus erythematosus and the risk of cardiovascular disease: results from the nurses' health study. Arthritis Rheum. 2009;61(10):1396–402. Epub 2009/10/01. PubMed Central PMCID: PMC2909444. doi: 10.1002/art.24537 - DOI - PMC - PubMed
-
- Asanuma Y, Oeser A, Shintani AK, Turner E, Olsen N, Fazio S, et al. Premature coronary-artery atherosclerosis in systemic lupus erythematosus. N Engl J Med. 2003;349(25):2407–15. doi: 10.1056/NEJMoa035611 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
