

Cost-effectiveness of nurse-led multifactorial care to prevent or postpone new disabilities in community-living older people: Results of a cluster randomized trial
- PMID: 28414806
- PMCID: PMC5393862
- DOI: 10.1371/journal.pone.0175272
Cost-effectiveness of nurse-led multifactorial care to prevent or postpone new disabilities in community-living older people: Results of a cluster randomized trial
Abstract
Objective: To evaluate the cost-effectiveness of nurse-led multifactorial care to prevent or postpone new disabilities in community-living older people in comparison with usual care.
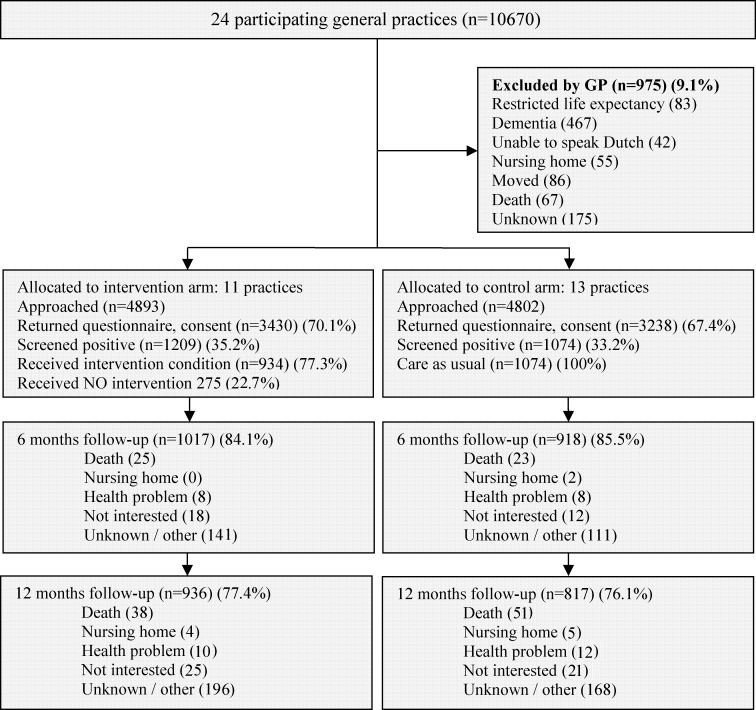
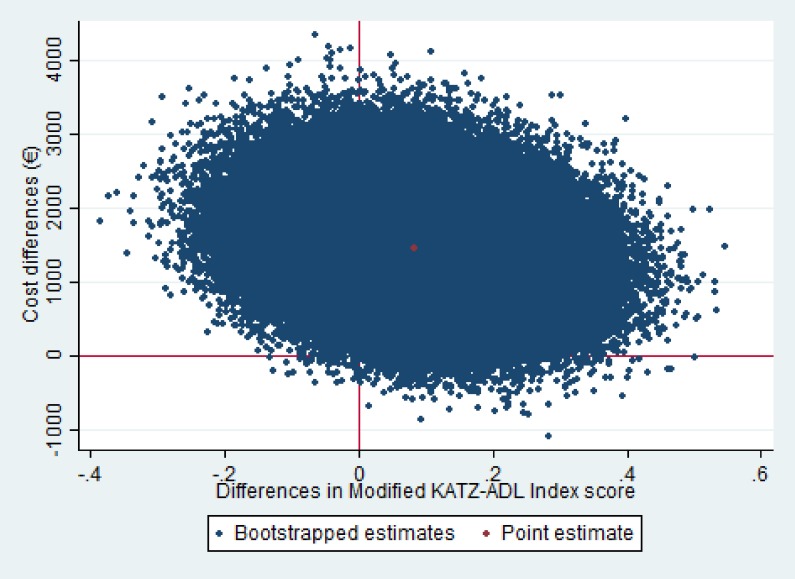
Methods: We conducted cost-effectiveness and cost-utility analyses alongside a cluster randomized trial with one-year follow-up. Participants were aged ≥ 70 years and at increased risk of functional decline. Participants in the intervention group (n = 1209) received a comprehensive geriatric assessment and individually tailored multifactorial interventions coordinated by a community-care registered nurse with multiple follow-up visits. The control group (n = 1074) received usual care. Costs were assessed from a healthcare perspective. Outcome measures included disability (modified Katz-Activities of Daily Living (ADL) index score), and quality-adjusted life-years (QALYs). Statistical uncertainty surrounding Incremental Cost-Effectiveness Ratios (ICERs) was estimated using bootstrapped bivariate regression models while adjusting for confounders.
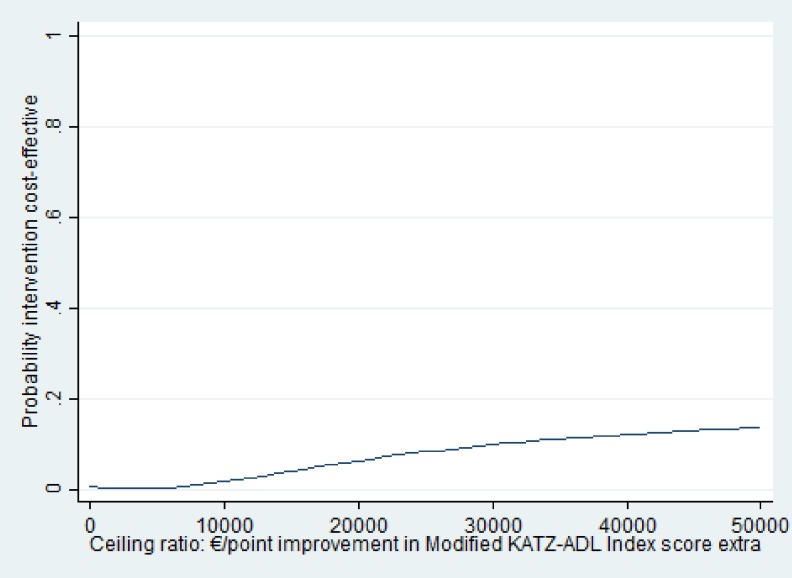
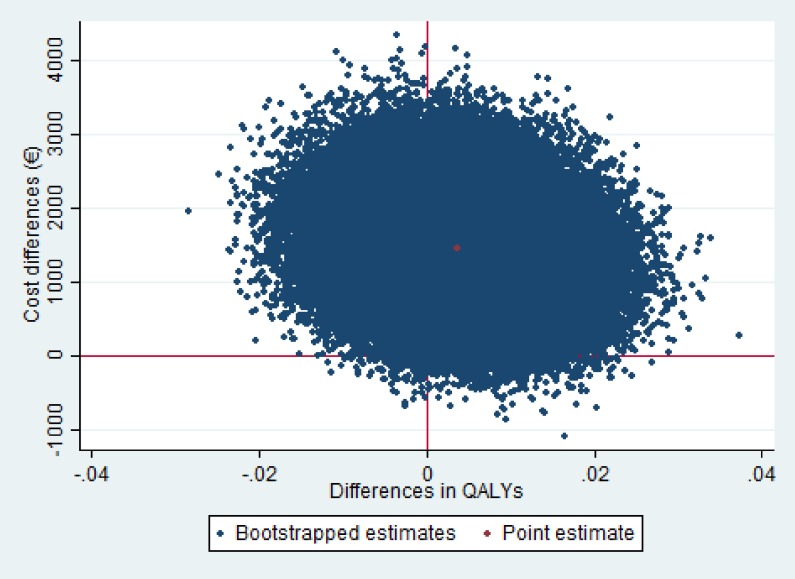
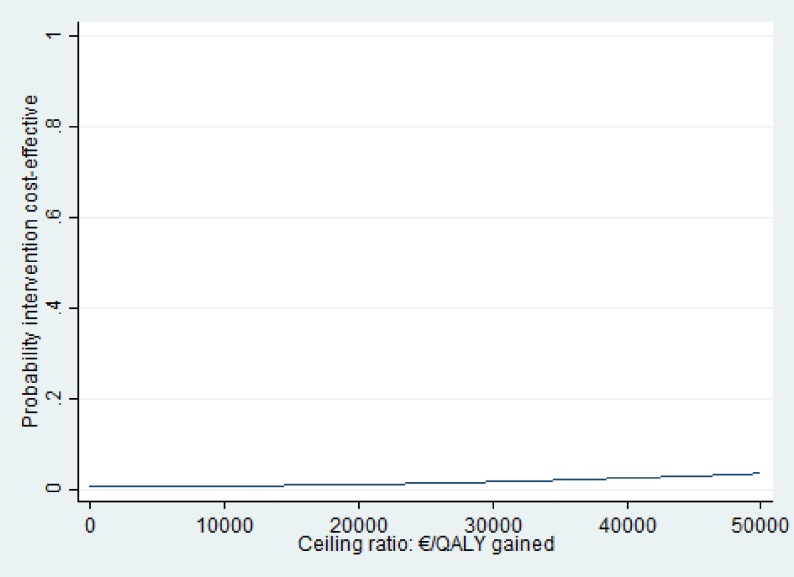
Results: There were no statistically significant differences in Katz-ADL index score and QALYs between the two groups. Total mean costs were significantly higher in the intervention group (EUR 6518 (SE 472) compared with usual care (EUR 5214 (SE 338); adjusted mean difference €1457 (95% CI: 572; 2537). Cost-effectiveness acceptability curves showed that the maximum probability of the intervention being cost-effective was 0.14 at a willingness to pay (WTP) of EUR 50,000 per one point improvement on the Katz-ADL index score and 0.04 at a WTP of EUR 50,000 per QALY gained.
Conclusion: The current intervention was not cost-effective compared to usual care to prevent or postpone new disabilities over a one-year period. Based on these findings, implementation of the evaluated multifactorial nurse-led care model is not to be recommended.
Conflict of interest statement
Figures
References
-
- Fried LP, Ferrucci L, Darer J, Williamson JD, Anderson G. Untangling the concepts of disability, frailty, and comorbidity: implications for improved targeting and care. The journals of gerontology Series A, Biological sciences and medical sciences. 2004;59(3):255–63. Epub 2004/03/20. - PubMed
-
- Beaton K, McEvoy C, Grimmer K. Identifying indicators of early functional decline in community-dwelling older people: A review. Geriatrics & gerontology international. 2014. Epub 2014/10/11. - PubMed
-
- Groessl EJ, Kaplan RM, Rejeski WJ, Katula JA, King AC, Frierson G, et al. Health-related quality of life in older adults at risk for disability. American journal of preventive medicine. 2007;33(3):214–8. PubMed Central PMCID: PMC1995005. doi: 10.1016/j.amepre.2007.04.031 - DOI - PMC - PubMed
-
- Hardy SE, Allore HG, Guo Z, Dubin JA, Gill TM. The effect of prior disability history on subsequent functional transitions. JGerontolA BiolSciMedSci. 2006;61(3):272–7. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
