

Definitive radiochemotherapy versus surgery within multimodality treatment in stage III non-small cell lung cancer (NSCLC) - a cumulative meta-analysis of the randomized evidence
- PMID: 28415831
- PMCID: PMC5522187
- DOI: 10.18632/oncotarget.16471
Definitive radiochemotherapy versus surgery within multimodality treatment in stage III non-small cell lung cancer (NSCLC) - a cumulative meta-analysis of the randomized evidence
Abstract
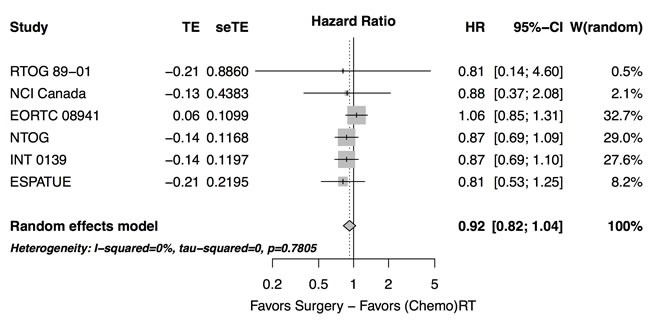
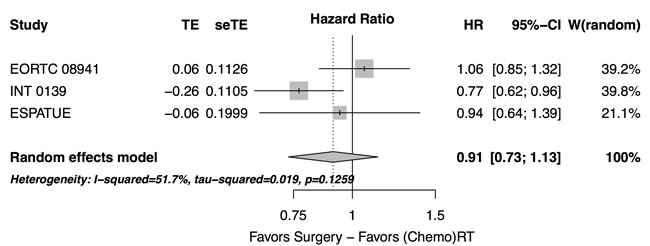
Randomized trials were analyzed comparing surgery with definitive radiotherapy as local curative treatment options within the framework of different multimodality treatments for patients with locally advanced non-small cell lung cancer (NSCLC). Endpoints for comparison of treatment results were overall survival, progression-free survival, and toxicity.Hazard ratios (HR) were taken to measure treatment effects and pooled using a random effects model.Overall survival was not significantly different between surgical and definitive radiotherapy arms (HR=0.92 [95%CI 0.82-1.04], p=0.19, χ2-test). There was heterogeneity with respect to survival at 2 years (p<0.0001, Cochran Mantel Haenszel (CMH)-test). Latter trials using concurrent radiochemotherapy (ccRT/CT) showed better survival at 2 years (risk ratio of death=0.80 [95%CI 0.73-0.88], p<0.0001, CMH-test). In the ccRT/CT trials, survival in the surgical arms tended to have an excess early mortality before 6 months of follow-up and a lesser hazard rate in comparison to definitive ccRT/CT thereafter (HR=0.78 [95%CI 0.63-0.98]). Over all trials, treatment associated mortality was higher in the surgical arms (risk ratio=3.56 [95% CI: 1.65-7.72], p=0.0005, CMH test). With respect to progression-free survival, no significant differences were found (HR=0.91 [95%CI: 0.73 - 1.13]), although the largest conducted trial found an advantage for the surgical arm (HR=0.77 [95%CI: 0.62-0.96]).Induction therapy followed by resection or definitive radiochemotherapy represent valuable curative treatment options for patients with stage III NSCLC, the individual treatment choice deserves careful interdisciplinary evaluation and counseling. Based on the broad heterogeneity of patient groups in these stages further research on predictive factors supporting individual therapy selection is necessary.
Keywords: NSCLC; meta-analysis; radiochemotherapy; trimodality.
Conflict of interest statement
Christoph Pöttgen: Honoraria: Roche.
Martin Stuschke, Georgios Stamatis: No relationship to disclose.
Wilfried Eberhardt:
Honoraria: Eli Lilly, Boehringer Ingelheim, Pfizer, Novartis, Roche, Merck, Bristol-Myers Squibb, Amgen, GlaxoSmithKline, Aestellas, Bayer, Teva, Merck Serono, Daichi Sankyo, Hexal
Consulting or Advisory Role: Eli Lilly, Boehringer Ingelheim, Novartis, Pfizer, Roche, Merck, Bristol-Myers Squibb, Aestellas, Bayer, Teva, Daichi Sankyo
Research Funding: Eli Lilly (Inst)
Figures
Similar articles
-
Meta-analysis of concomitant versus sequential radiochemotherapy in locally advanced non-small-cell lung cancer.J Clin Oncol. 2010 May 1;28(13):2181-90. doi: 10.1200/JCO.2009.26.2543. Epub 2010 Mar 29. J Clin Oncol. 2010. PMID: 20351327 Review.
-
The impact of extent and location of mediastinal lymph node involvement on survival in Stage III non-small cell lung cancer patients treated with definitive radiotherapy.Int J Radiat Oncol Biol Phys. 2012 May 1;83(1):340-7. doi: 10.1016/j.ijrobp.2011.05.070. Epub 2011 Nov 19. Int J Radiat Oncol Biol Phys. 2012. PMID: 22104359
-
Long-term survival of patients with central or > 7 cm T4 N0/1 M0 non-small-cell lung cancer treated with definitive concurrent radiochemotherapy in comparison to trimodality treatment.Radiat Oncol. 2022 Jul 16;17(1):126. doi: 10.1186/s13014-022-02080-9. Radiat Oncol. 2022. PMID: 35842712 Free PMC article.
-
Long-term results in patients with pathological complete response after induction radiochemotherapy followed by surgery for locally advanced non-small-cell lung cancer.Eur J Cardiothorac Surg. 2013 Mar;43(3):e71-81. doi: 10.1093/ejcts/ezs622. Epub 2013 Jan 4. Eur J Cardiothorac Surg. 2013. PMID: 23293319
-
Patient subsets benefiting from adjuvant therapy following surgical resection of non-small cell lung cancer.Clin Cancer Res. 2005 Jul 1;11(13 Pt 2):5022s-5026s. doi: 10.1158/1078-0432.CCR-05-9001. Clin Cancer Res. 2005. PMID: 16000607 Review.
Cited by
-
Surgery for stage IIIA-N2 non-small cell lung cancer: the jury is still out!J Thorac Dis. 2019 May;11(Suppl 9):S1153-S1156. doi: 10.21037/jtd.2019.04.36. J Thorac Dis. 2019. PMID: 31245070 Free PMC article. No abstract available.
-
Interdisciplinary multimodality management of stage III nonsmall cell lung cancer.Eur Respir Rev. 2019 Jul 8;28(152):190024. doi: 10.1183/16000617.0024-2019. Print 2019 Jun 30. Eur Respir Rev. 2019. PMID: 31285288 Free PMC article. Review.
-
Hesperetin reverses P‑glycoprotein‑mediated cisplatin resistance in DDP‑resistant human lung cancer cells via modulation of the nuclear factor‑κB signaling pathway.Int J Mol Med. 2020 Apr;45(4):1213-1224. doi: 10.3892/ijmm.2020.4485. Epub 2020 Feb 5. Int J Mol Med. 2020. PMID: 32124932 Free PMC article.
-
Postoperative radiotherapy improves survival in completely resected non-small cell lung cancer with pathologic N2 stage IIIA and positive lymph node count greater than one: a SEER-based retrospective cohort study.Front Surg. 2025 Feb 4;11:1506854. doi: 10.3389/fsurg.2024.1506854. eCollection 2024. Front Surg. 2025. PMID: 39968112 Free PMC article.
-
Resectable IIIA-N2 Non-Small-Cell Lung Cancer (NSCLC): In Search for the Proper Treatment.Cancers (Basel). 2020 Jul 25;12(8):2050. doi: 10.3390/cancers12082050. Cancers (Basel). 2020. PMID: 32722386 Free PMC article. Review.
References
-
- Goldstraw P, Chansky K, Crowley J, Rami-Porta R, Asamura H, Eberhardt WE, Nicholson AG, Groome P, Mitchell A, Bolejack V. International Association for the Study of Lung Cancer Staging and Prognostic Factors Committee, Advisory Boards, and Participating Institutions. The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer. J Thorac Oncol. 2016;11:39–51. doi: 10.1016/j.jtho.2015.09.009. - DOI - PubMed
-
- Robinson LA, Ruckdeschel JC, Wagner H, Jr, Stevens CW, American College of Chest Physicians Treatment of non-small cell lung cancer-stage IIIA: ACCP evidence-based guidelines (2nd edition) Chest. 2007;132(suppl 3):243S–65S. - PubMed
-
- Ramnath N, Dilling TJ, Harris LJ, Kim AW, Michaud GC, Balekian AA, Diekemper R, Detterbeck FC, Arenberg DA. Treatment of stage III non-small cell lung cancer: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013;(Suppl):e314S–40S. doi: 10.1378/chest.12-2360. - DOI - PubMed
-
- Ettinger DS, Wood DE, Akerley W, Bazhenova LA, Borghaei H, Camidge DR, Cheney RT, Chirieac LR, D’Amico TA, Dilling TJ, Dobelbower MC, Govindan R, Hennon M, et al. Non-Small Cell Lung Cancer, Version 04.2016. https://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf
-
- Eberhardt WE, De Ruysscher D, Weder W, Le Péchoux C, De Leyn P, Hoffmann H, Westeel V, Stahel R, Felip E, Peters S. Panel Members. 2nd ESMO Consensus Conference in Lung Cancer: locally advanced stage III non-small-cell lung cancer. Ann Oncol. 2015;26:1573–88. doi: 10.1093/annonc/mdv187. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
