

Clinical study of children with Takayasu arteritis: a retrospective study from a single center in China
- PMID: 28416004
- PMCID: PMC5393038
- DOI: 10.1186/s12969-017-0164-2
Clinical study of children with Takayasu arteritis: a retrospective study from a single center in China
Abstract
Background: Delayed diagnosis of childhood Takayasu arteritis (TA) is common due to its atypical symptoms. The objective of the present study was to summarize the clinical features of childhood TA to raise awareness and improve management.
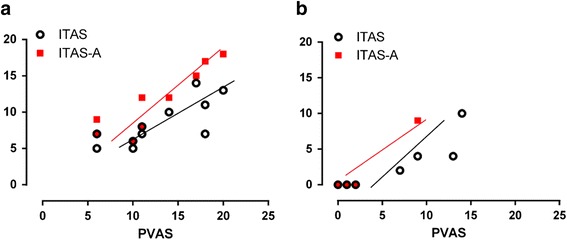
Methods: Eleven children diagnosed with TA at our hospital were enrolled. Clinical information, diagnosis, treatment, and outcome were then examined retrospectively. The Pediatric Vasculitis Activity Score (PVAS) and the Indian Takayasu Clinical Activity Score (ITAS2010) were used to assess disease activity.
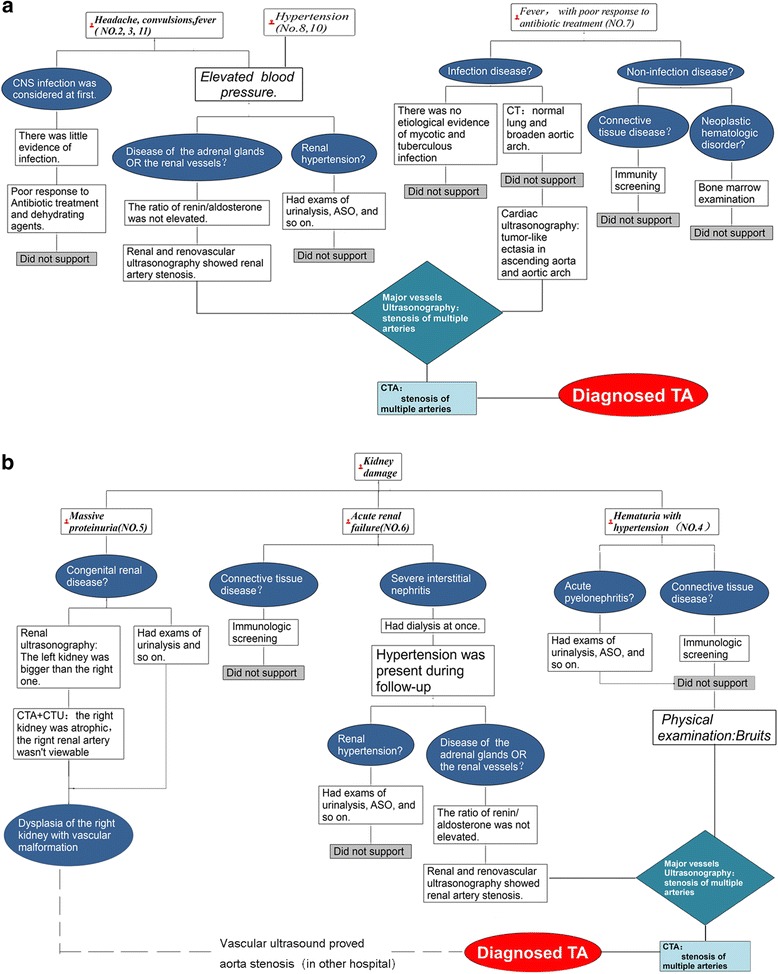
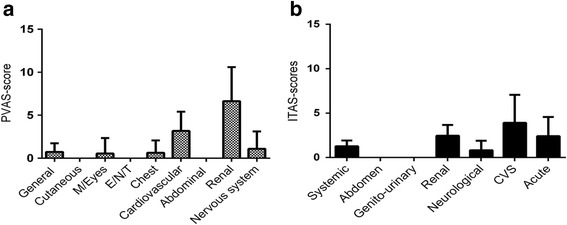
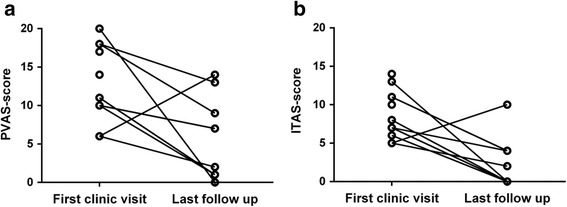
Results: Male-to-female ratio was 4:7. The mean age was 9.4 (1.4-14) years and the average time to diagnosis was 40.6 days (12-90 days). All patients suffered from hypertension and few had immunologic abnormalities. Two patients had low levels of autoantibodies and one had elevated immunoglobulin E levels. Aberrant (elevated) laboratory parameters included erythrocyte sedimentation rate (ESR) (9/10 patients, 90.0%), protein excretion (8/9 patients, 88.9%), renin-angiotensin-aldosterone system (RAAS) activity (5/5 patients, 100.0%), and serum lipid levels (3/5 patients, 60%). The common onset patterns were headache with convulsions (27.2%) and kidney damage (27.2%). The abdominal aorta (81.8%) and renal artery (72.7%) were the most commonly involved vessels. At presentation, the mean PVAS and ITAS2010 scores were 12.1 (6-26)/63 and 9.7 (5-14)/57, respectively. All patients were treated with glucocorticoids and antihypertensive agents; two underwent renal artery stent placement.
Conclusion: The diagnosis of TA should be considered in patients with pediatric hypertension and high expression of inflammatory markers or abnormal urine results. Doppler ultrasonography of major vessels may be helpful. PVAS and ITAS2010 both help to evaluate disease activity, and the PVAS is recommended for patients with kidney damage. Glucocorticoid and antihypertensive agents are effective. Interventional therapy can be an option for patients with persistent hypertension.
Keywords: Diagnostic framework; Disease activity score; Hypertension; Pediatric rheumatology; Takayasu’s arteritis; Ultrasonography.
Figures
References
-
- Clemente G, Hilario MO, Lederman H, et al. Takayasu arteritis in a Brazilian multicenter study: children with a longer diagnosis delay than adolescents. Clin Exp Rheumatol. 2014;32(3 Suppl 82):S128–33. - PubMed
-
- Ozen S, Pistorio A, Iusan SM, et al. EULAR/PRINTO/PRES criteria for Henoch-Schönlein purpura, childhood polyarteritis nodosa, childhood Wegener granulomatosis and childhood Takayasu arteritis: Ankara 2008. Part II: Final classification criteria. Ann Rheum Dis. 2010;69(5):798–806. doi: 10.1136/ard.2009.116657. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
