

Specific or general exercise strategy for subacromial impingement syndrome-does it matter? A systematic literature review and meta analysis
- PMID: 28416022
- PMCID: PMC5393017
- DOI: 10.1186/s12891-017-1518-0
Specific or general exercise strategy for subacromial impingement syndrome-does it matter? A systematic literature review and meta analysis
Abstract
Background: Exercise is frequently suggested as a treatment option for patients presenting with symptoms of subacromial impingement syndrome. Some would argue implementing a specific exercise strategy with special focus on correction of kinematic deficits would be superior to general exercise strategy. There is however a lack of evidence comparing such exercise strategies to determine which is the most effective in the treatment of subacromial impingement syndrome. The aim of this review is to evaluate whether implementing specific exercise strategies involving resistive exercises are more effective than a general exercise strategy for the treatment of patients with subacromial impingement syndrome.
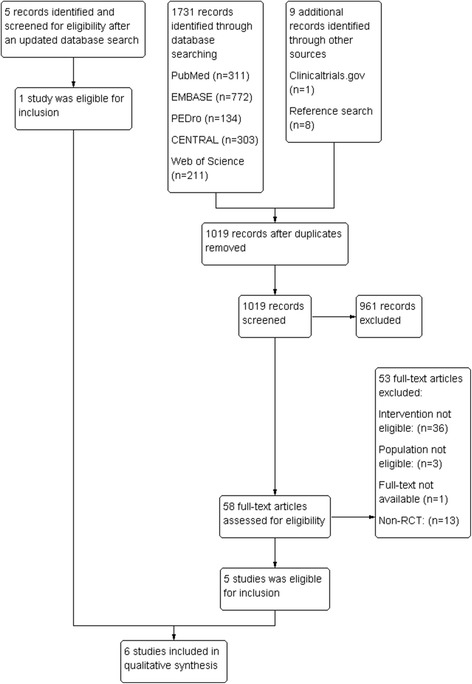
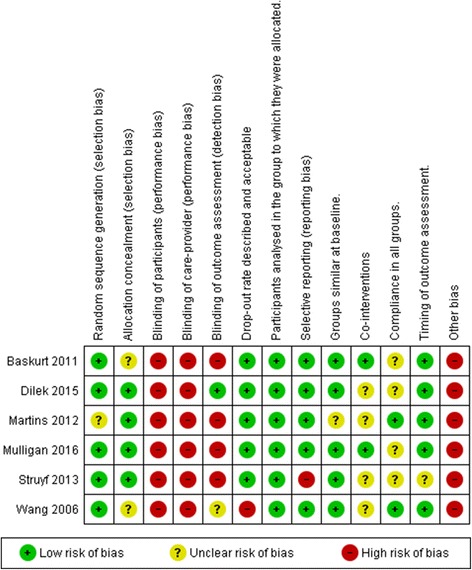
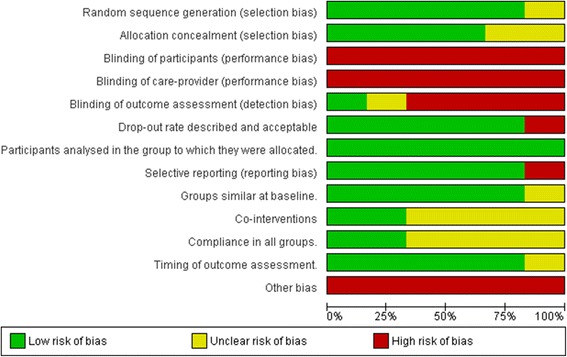
Methods: Randomized controlled trials were identified through an electronic search on PubMed/MEDLINE, EMBASE, Cochrane Central Register of Controlled Trials, Web of Science and PEDro. In addition, article reference lists and Clinicaltrials.gov were searched. Studies were considered eligible if they included interventions with resistive specific exercises as compared to general resistance exercise. Four reviewers assessed risk of bias and methodological quality guided by Cochrane recommendations. Results were synthesised qualitatively or quantitatively, where appropriate.
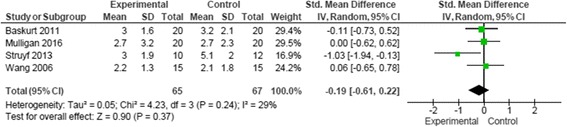
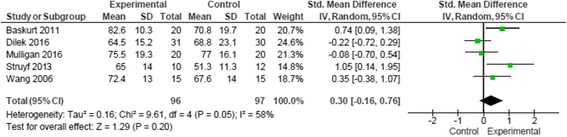
Results: Six randomized controlled trials were included with 231 participants who experienced symptoms of subacromial impingement syndrome. Four studies evaluated the effectiveness of specific scapular exercise strategy and two studies evaluated the effectiveness of specific proprioceptive strategy. Five studies were of moderate quality and one study was of low quality. No consistent statistical significant differences in outcomes between treatment groups were reported in the studies. Standardized mean difference (SMD) for pain was SMD -0.19 (95% CI -0.61, 0.22) and SMD 0.30 (95% CI -0.16, 0.76) for function.
Conclusions: There is insufficient evidence to support or refute the effectiveness of specific resistive exercise strategies in the rehabilitation of subacromial impingement syndrome. More high quality research is needed to accurately assess this. This review provides suggestions on how to improve the methodological design of future studies in this area.
Keywords: Function; Impingement; Pain; Physiotherapy; Shoulder; Subacromial; Training.
Figures
References
-
- Neer CS. Impingement lesions. Clin Orthop Relat Res. 1983;173:70–77. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
