

Flow Mediated Dilatation and Progression of Abdominal Aortic Aneurysms
- PMID: 28416190
- PMCID: PMC5496669
- DOI: 10.1016/j.ejvs.2017.03.001
Flow Mediated Dilatation and Progression of Abdominal Aortic Aneurysms
Abstract
Objective/background: Biomarker(s) for prediction of the future progression rate of abdominal aortic aneurysms (AAA) may be useful to stratify the management of individual patients. AAAs are associated with features of systemic inflammation and endothelial dysfunction. Flow mediated dilatation (FMD) of the brachial artery is a recognised non-invasive measurement for endothelial function. We hypothesised that FMD is a potential biomarker of AAA progression and reflects the temporal changes of endothelial function during AAA progression.
Methods: In a prospectively recruited cohort of patients with AAAs (Oxford Abdominal Aortic Aneurysm Study), AAA size was recorded by antero-posterior diameter (APD) (outer to outer) on ultrasound. Annual AAA progression was calculated by (ΔAPD/APD at baseline)/(number of days lapsed/365 days). FMD was assessed at the same time as AAA size measurement. Analyses of data were performed in the overall cohort, and further in subgroups of AAA by size (small: 30-39 mm; moderate: 40-55 mm; large: > 55 mm).
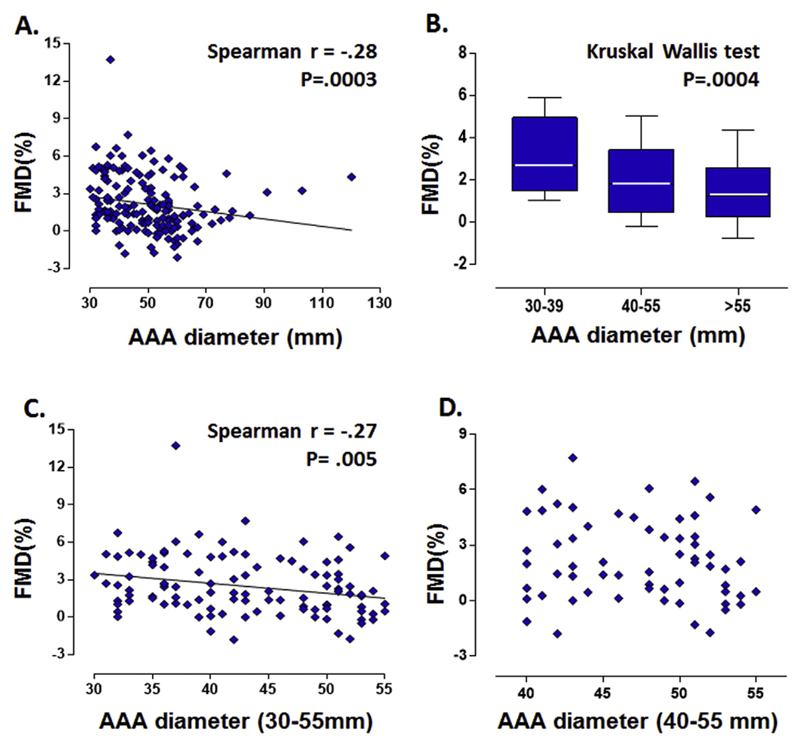
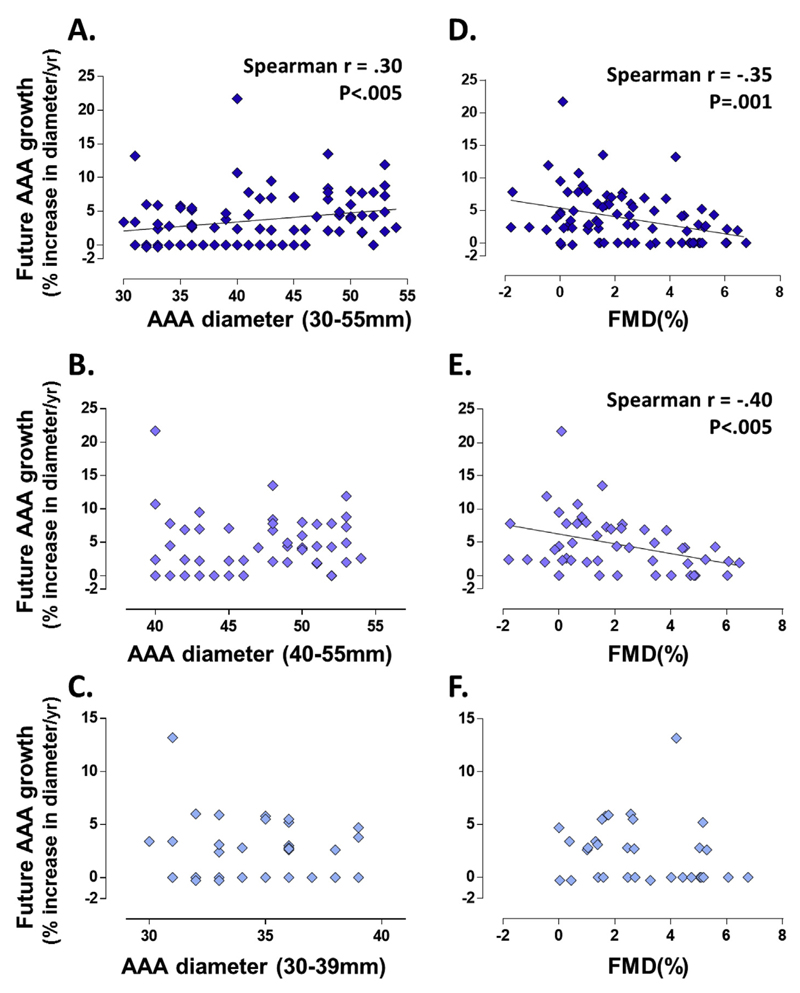
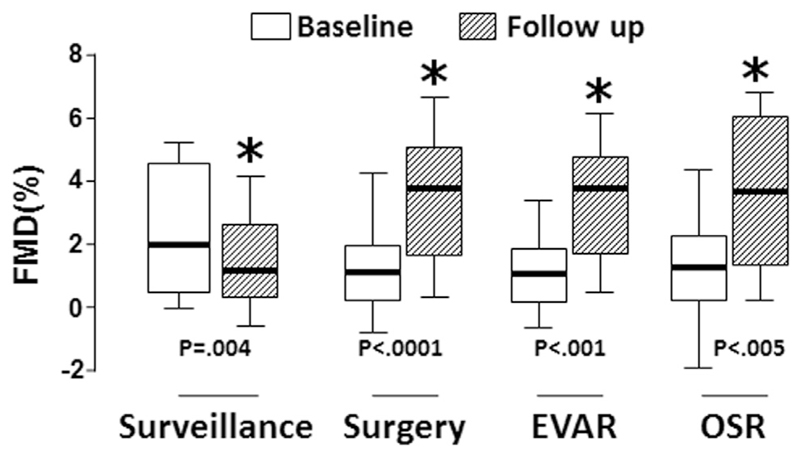
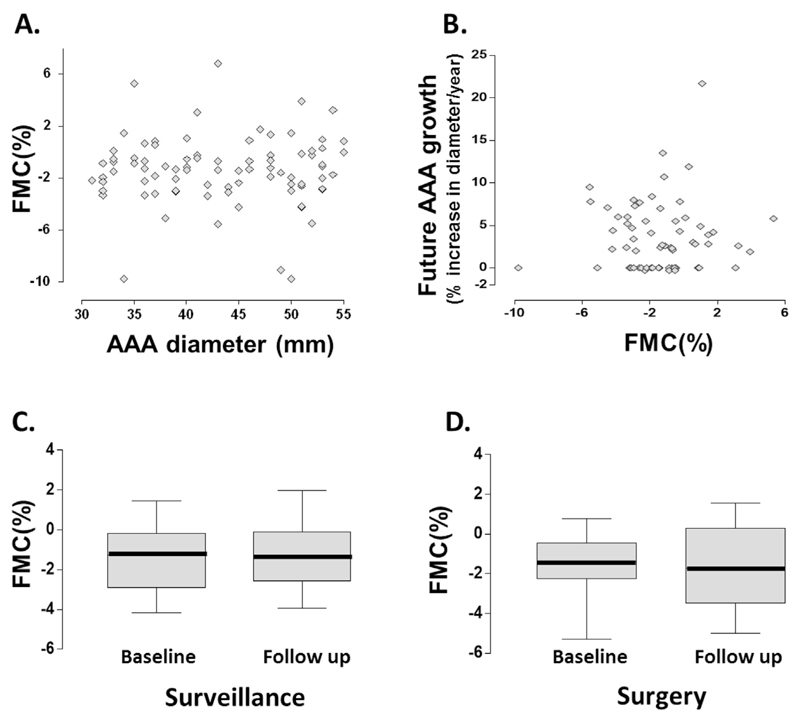
Results: FMD is inversely correlated with the diameter of AAAs in all patients (n=162, Spearman's r=-.28, p<.001). FMD is inversely correlated with AAA diameter progression in the future 12 months (Spearman's r=-.35, p=.001), particularly in the moderate size group. Furthermore, FMD deteriorates during the course of AAA surveillance (from a median of 2.0% at baseline to 1.2% at follow-up; p=.004), while surgical repair of AAAs (n=50 [open repair n=22, endovascular repair n=28)] leads to an improvement in FMD (from 1.1% pre-operatively to 3.8% post-operatively; p<.001), irrespective of the type of surgery.
Conclusion: FMD is inversely correlated with future AAA progression in humans. FMD deteriorates during the natural history of AAA, and is improved by surgery. The utility of FMD as a potential biomarker in the context of AAA warrants further investigation.
Keywords: AAA Progression; Abdominal aortic aneurysm; Biomarkers; Flow mediated dilatation.
Copyright © 2017 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
None.
Figures
Comment in
-
Commentary on "Flow Mediated Dilatation and the Progression of Abdominal Aortic Aneurysms".Eur J Vasc Endovasc Surg. 2017 Jun;53(6):830. doi: 10.1016/j.ejvs.2017.03.011. Epub 2017 Apr 8. Eur J Vasc Endovasc Surg. 2017. PMID: 28400092 No abstract available.
References
-
- Chaikof EL, Brewster DC, Dalman RL, Makaroun MS, Illig KA, Sicard GA, et al. SVS practice guidelines for the care of patients with an abdominal aortic aneurysm: executive summary. J Vasc Surg. 2009;50:880–96. - PubMed
-
- Rutherford RB. Open versus endovascular stent graft repair for abdominal aortic aneurysms: an historical view. Semin Vasc Surg. 2012;25:39–48. - PubMed
-
- Medina F, de Haro J, Florez A, Acin F. Relationship between endothelial dependent vasodilation and size of abdominal aortic aneurysms. Ann Vasc Surg. 2010;24:752–7. - PubMed
-
- Sung SH, Wu TC, Chen JS, Chen YH, Huang PH, Lin SJ, et al. Reduced number and impaired function of circulating endothelial progenitor cells in patients with abdominal aortic aneurysm. Int J Cardiol. 2013;168:1070–7. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
